

Effects of the Lower Airway Secretions on Airway Opening Pressures and Suction Pressures in Critically Ill COVID-19 Patients: A Computational Simulation
- PMID: 33078367
- PMCID: PMC7571532
- DOI: 10.1007/s10439-020-02648-0
Effects of the Lower Airway Secretions on Airway Opening Pressures and Suction Pressures in Critically Ill COVID-19 Patients: A Computational Simulation
Abstract
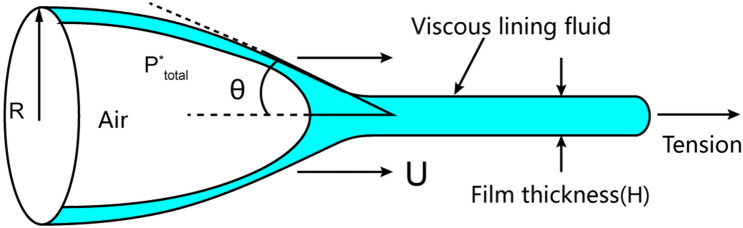
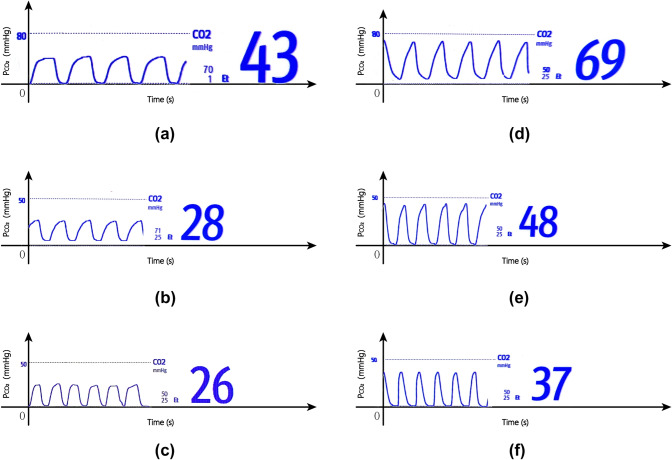
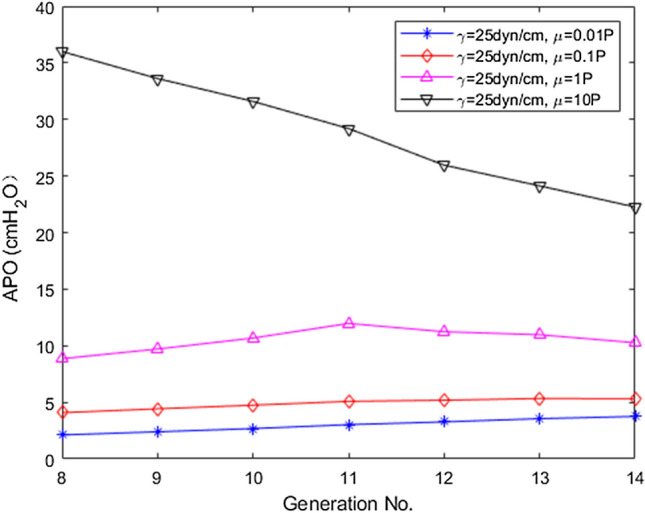
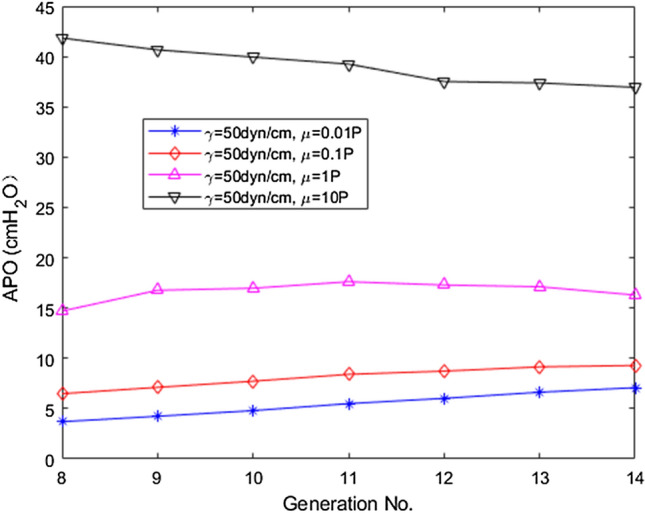
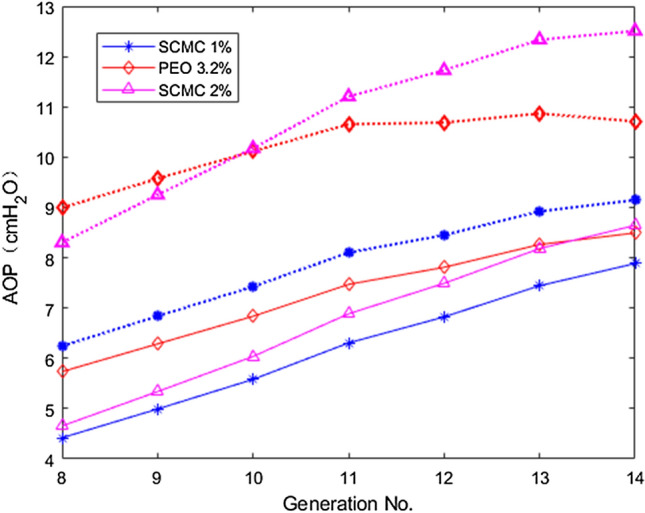
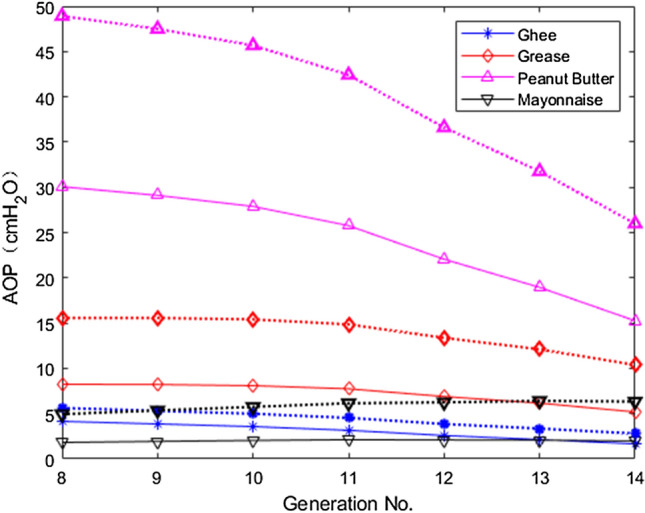
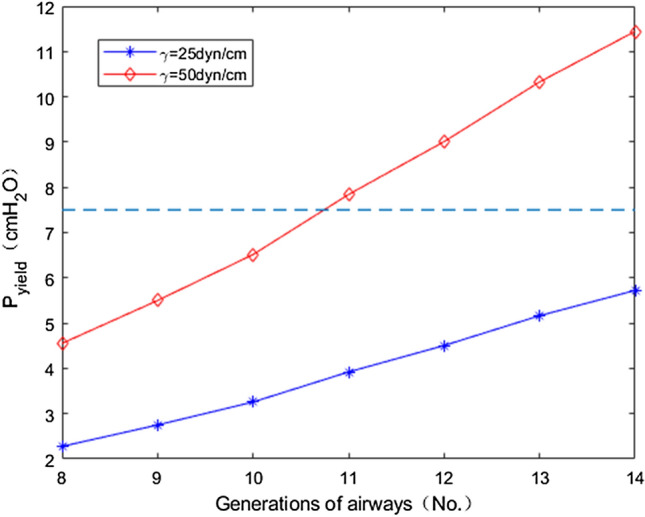
In patients with critically ill COVID-19 pneumonia, lower airways are filled with plenty of highly viscous exudates or mucus, leading to airway occlusion. The estimation of airway opening pressures and effective mucus clearance are therefore two issues that clinicians are most concerned about during mechanical ventilation. In this study we retrospectively analyzed respiratory data from 24 critically ill patients with COVID-19 who received invasive mechanical ventilation and recruitment maneuver at Jinyintan Hospital in Wuhan, China. Among 24 patients, the mean inspiratory plateau pressure was 52.4 ± 4.4 cmH2O (mean ± [SD]). Particularly, the capnograms presented an upward slope during the expiratory plateau, indicting the existence of airway obstruction. A computational model of airway opening was subsequently introduced to investigate possible fluid dynamic mechanisms for the extraordinarily high inspiratory plateau pressures among these patients. Our simulation results showed that the predicted airway opening pressures could be as high as 40-50 cmH2O and the suction pressure could exceed 20 kPa as the surface tension and viscosity of secretion simulants markedly increased, likely causing the closures of the distal airways. We concluded that, in some critically ill patients with COVID-19, limiting plateau pressure to 30 cmH2O may not guarantee the opening of airways due to the presence of highly viscous lower airway secretions, not to mention spontaneous inspiratory efforts. Active airway humidification and effective expectorant drugs are therefore strongly recommended during airway management.
Keywords: Airway mucus; Airway opening pressure; Coronavirus disease 2019; Endotracheal suctioning; Respiratory mechanics.
Figures
Similar articles
-
Airway resistance variation correlates with prognosis of critically ill COVID-19 patients: A computational fluid dynamics study.Comput Methods Programs Biomed. 2021 Sep;208:106257. doi: 10.1016/j.cmpb.2021.106257. Epub 2021 Jun 25. Comput Methods Programs Biomed. 2021. PMID: 34245951 Free PMC article.
-
Positive end-expiratory pressure in COVID-19-related ARDS: Do not forget the airway closure.J Crit Care. 2021 Aug;64:141-143. doi: 10.1016/j.jcrc.2021.04.005. Epub 2021 Apr 20. J Crit Care. 2021. PMID: 33906102 Free PMC article.
-
Esophageal pressures in acute lung injury: do they represent artifact or useful information about transpulmonary pressure, chest wall mechanics, and lung stress?J Appl Physiol (1985). 2010 Mar;108(3):515-22. doi: 10.1152/japplphysiol.00835.2009. Epub 2009 Dec 17. J Appl Physiol (1985). 2010. PMID: 20019160 Free PMC article.
-
Ventilator strategies for posttraumatic acute respiratory distress syndrome: airway pressure release ventilation and the role of spontaneous breathing in critically ill patients.Curr Opin Crit Care. 2004 Dec;10(6):549-57. doi: 10.1097/01.ccx.0000145473.01597.13. Curr Opin Crit Care. 2004. PMID: 15616399 Review.
-
[High frequency jet ventilation combined with conventional mechanical ventilation in the treatment of adult respiratory distress syndrome].Ann Fr Anesth Reanim. 1995;14(3):276-88. doi: 10.1016/s0750-7658(95)80007-7. Ann Fr Anesth Reanim. 1995. PMID: 7486298 Review. French.
Cited by
-
Ventilation/perfusion mismatch is not the sole reason for hypoxaemia in early stage COVID-19 patients.Eur Respir Rev. 2022 Jun 28;31(164):210277. doi: 10.1183/16000617.0277-2021. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35768132 Free PMC article.
-
Publications About COVID-19 Research by the BME Community.Ann Biomed Eng. 2022 Dec;50(12):1701-1703. doi: 10.1007/s10439-022-03068-y. Epub 2022 Sep 6. Ann Biomed Eng. 2022. PMID: 36066782 Free PMC article. No abstract available.
-
Airway resistance variation correlates with prognosis of critically ill COVID-19 patients: A computational fluid dynamics study.Comput Methods Programs Biomed. 2021 Sep;208:106257. doi: 10.1016/j.cmpb.2021.106257. Epub 2021 Jun 25. Comput Methods Programs Biomed. 2021. PMID: 34245951 Free PMC article.
-
Application of an evidence-based, out-patient treatment strategy for COVID-19: Multidisciplinary medical practice principles to prevent severe disease.J Neurol Sci. 2021 Jul 15;426:117463. doi: 10.1016/j.jns.2021.117463. Epub 2021 Apr 20. J Neurol Sci. 2021. PMID: 33971376 Free PMC article. Review.
-
Sex differences in airway disease: estrogen and airway surface liquid dynamics.Biol Sex Differ. 2024 Jul 18;15(1):56. doi: 10.1186/s13293-024-00633-z. Biol Sex Differ. 2024. PMID: 39026347 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
