

The Role of Value-Based Payment in Promoting Innovation to Address Social Risks: A Cross-Sectional Study of Social Risk Screening by US Physicians
- PMID: 33078875
- PMCID: PMC7772636
- DOI: 10.1111/1468-0009.12480
The Role of Value-Based Payment in Promoting Innovation to Address Social Risks: A Cross-Sectional Study of Social Risk Screening by US Physicians
Abstract
Policy Points One of the most important possibilities of value-based payment is its potential to spur innovation in upstream prevention, such as attention to social needs that lead to poor health. Screening patients for social risks such as housing instability and food insecurity represents an early step physician practices can take to address social needs. At present, adoption of social risk screening by physician practices is linked with having high innovation capacity and focusing on low-income populations, but not exposure to value-based payment. Expanding social risk screening by physician practices may require standardization and technical assistance for practices that have less innovative capacity.
Context: One of the most important possibilities of value-based payment is its potential to spur innovation in upstream prevention, such as attention to social needs that lead to poor health. However, there is uncertainty about the conditions under which value-based payment will encourage health care providers to innovate to address upstream social risks.
Methods: We used the 2017-2018 National Survey of Healthcare Organizations and Systems (NSHOS), a nationally representative survey of physician practices (n = 2,178), to ascertain (1) the number of social risks for which practices systematically screen patients; (2) the extent of practices' participation in value-based payment models; and (3) measures of practices' capacity for innovation. We used multivariate regression models to examine predictors of social risk screening.
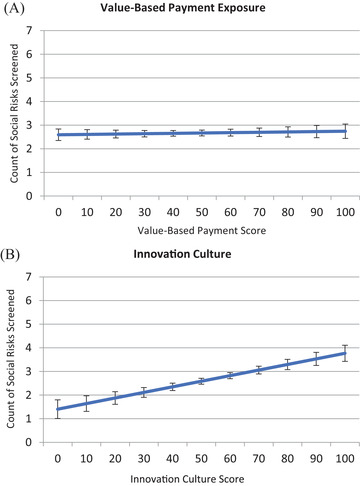
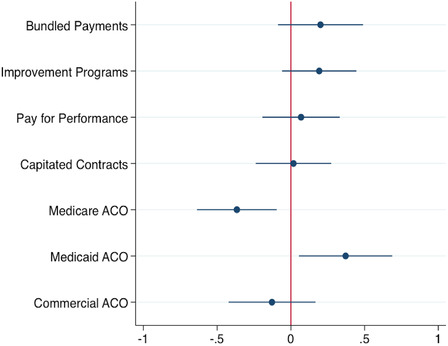
Findings: On average, physician practices systematically screened for 2.4 out of 7 (34%) social risks assessed by the survey. In the fully adjusted model, implementing social risk screening was not associated with the practices' overall exposure to value-based payment. Being in the top quartile on any of three innovation capacity scales, however, was associated with screening for 0.95 to 1.00 additional social risk (p < 0.001 for all three results) relative to the bottom quartile. In subanalysis examining specific payment models, participating in a Medicaid accountable care organization was associated with screening for 0.37 more social risks (p = 0.015). Expecting more exposure to accountable care in the future was associated with greater social risk screening, but the effect size was small compared with practices' capacity for innovation.
Conclusions: Our results indicate that implementation of social risk screening-an initial step in enhancing awareness of social needs in health care-is not associated with overall exposure to value-based payment for physician practices. Expanding social risk screening by physician practices may require standardized approaches and implementation assistance to reduce the level of innovative capacity required.
Keywords: implementation science; primary care; social determinants of health; social risk screening.
© 2020 Milbank Memorial Fund.
Figures
Comment in
-
In the December 2020 Issue of the Quarterly.Milbank Q. 2020 Dec;98(4):1027-1032. doi: 10.1111/1468-0009.12487. Milbank Q. 2020. PMID: 33377289 Free PMC article. No abstract available.
References
-
- Bachrach D, Pfister H, Wallis K, Lipson M. Addressing Patients’ Social Needs: An Emerging Business Case for Provider Investment. New York, NY: The Commonwealth Fund; 2014.
