

Lifetime Prevalence of Cervical Cancer Screening in 55 Low- and Middle-Income Countries
- PMID: 33079153
- PMCID: PMC7576410
- DOI: 10.1001/jama.2020.16244
Lifetime Prevalence of Cervical Cancer Screening in 55 Low- and Middle-Income Countries
Abstract
Importance: The World Health Organization is developing a global strategy to eliminate cervical cancer, with goals for screening prevalence among women aged 30 through 49 years. However, evidence on prevalence levels of cervical cancer screening in low- and middle-income countries (LMICs) is sparse.
Objective: To determine lifetime cervical cancer screening prevalence in LMICs and its variation across and within world regions and countries.
Design, setting, and participants: Analysis of cross-sectional nationally representative household surveys carried out in 55 LMICs from 2005 through 2018. The median response rate across surveys was 93.8% (range, 64.0%-99.3%). The population-based sample consisted of 1 136 289 women aged 15 years or older, of whom 6885 (0.6%) had missing information for the survey question on cervical cancer screening.
Exposures: World region, country; countries' economic, social, and health system characteristics; and individuals' sociodemographic characteristics.
Main outcomes and measures: Self-report of having ever had a screening test for cervical cancer.
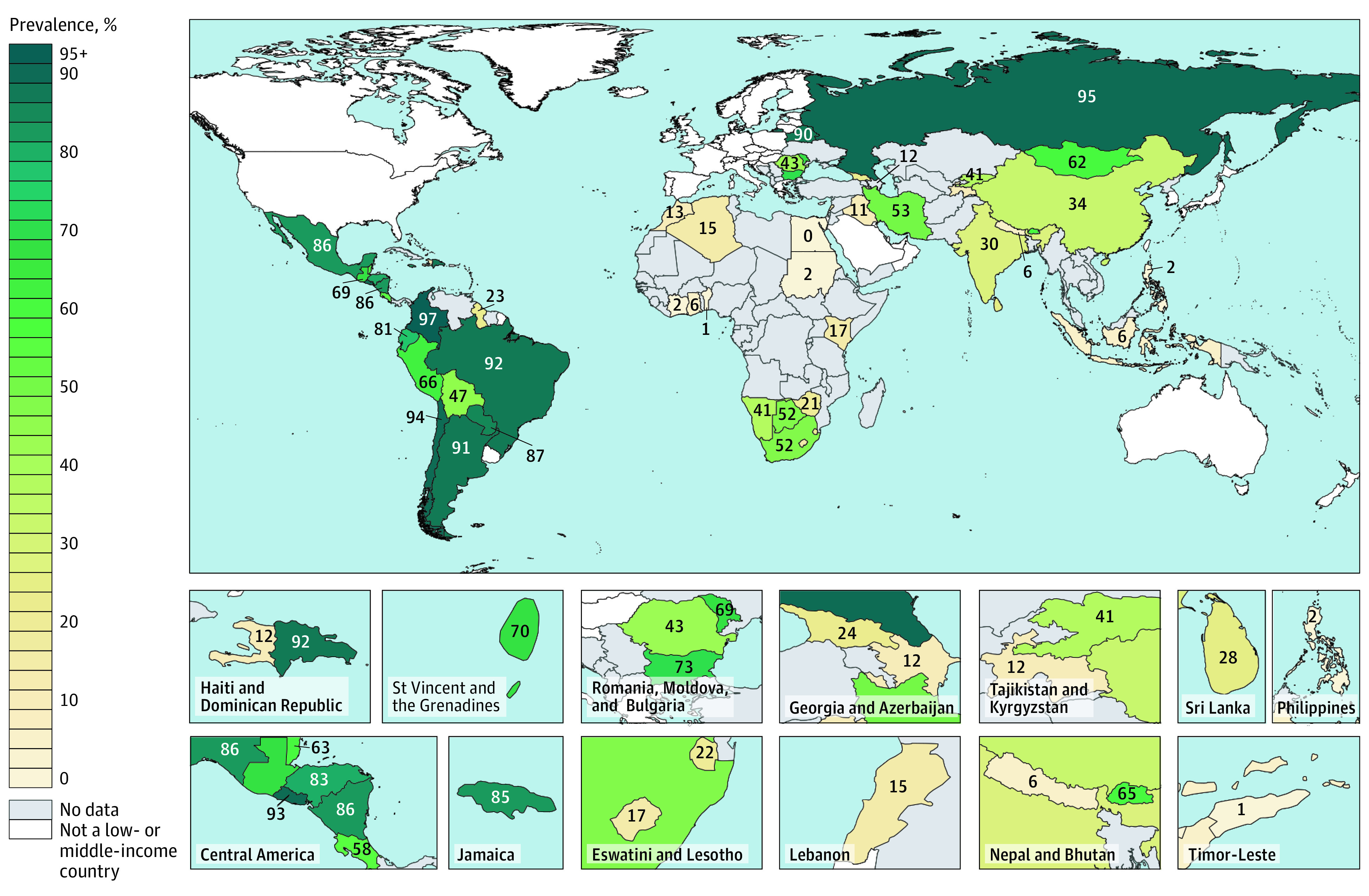
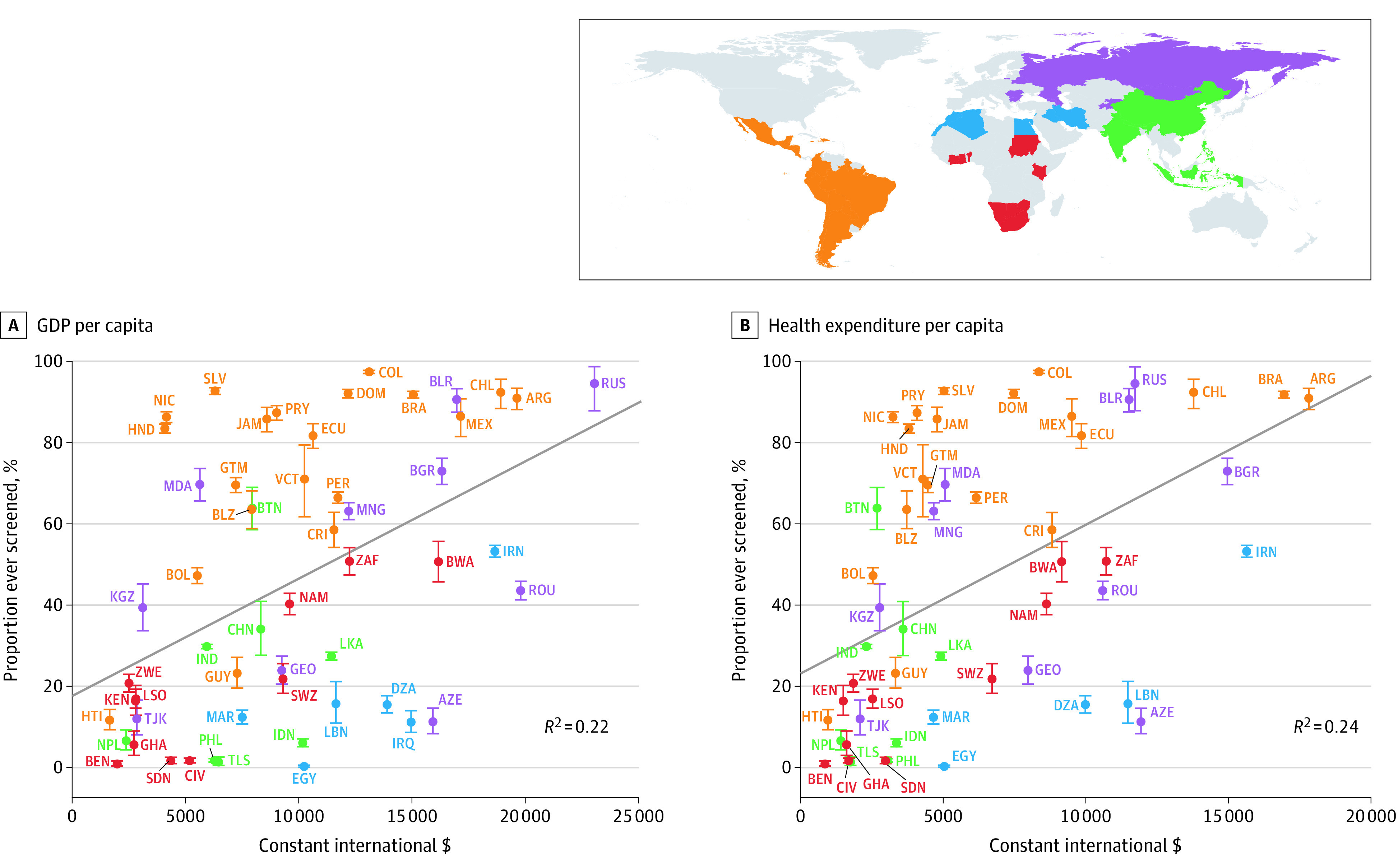
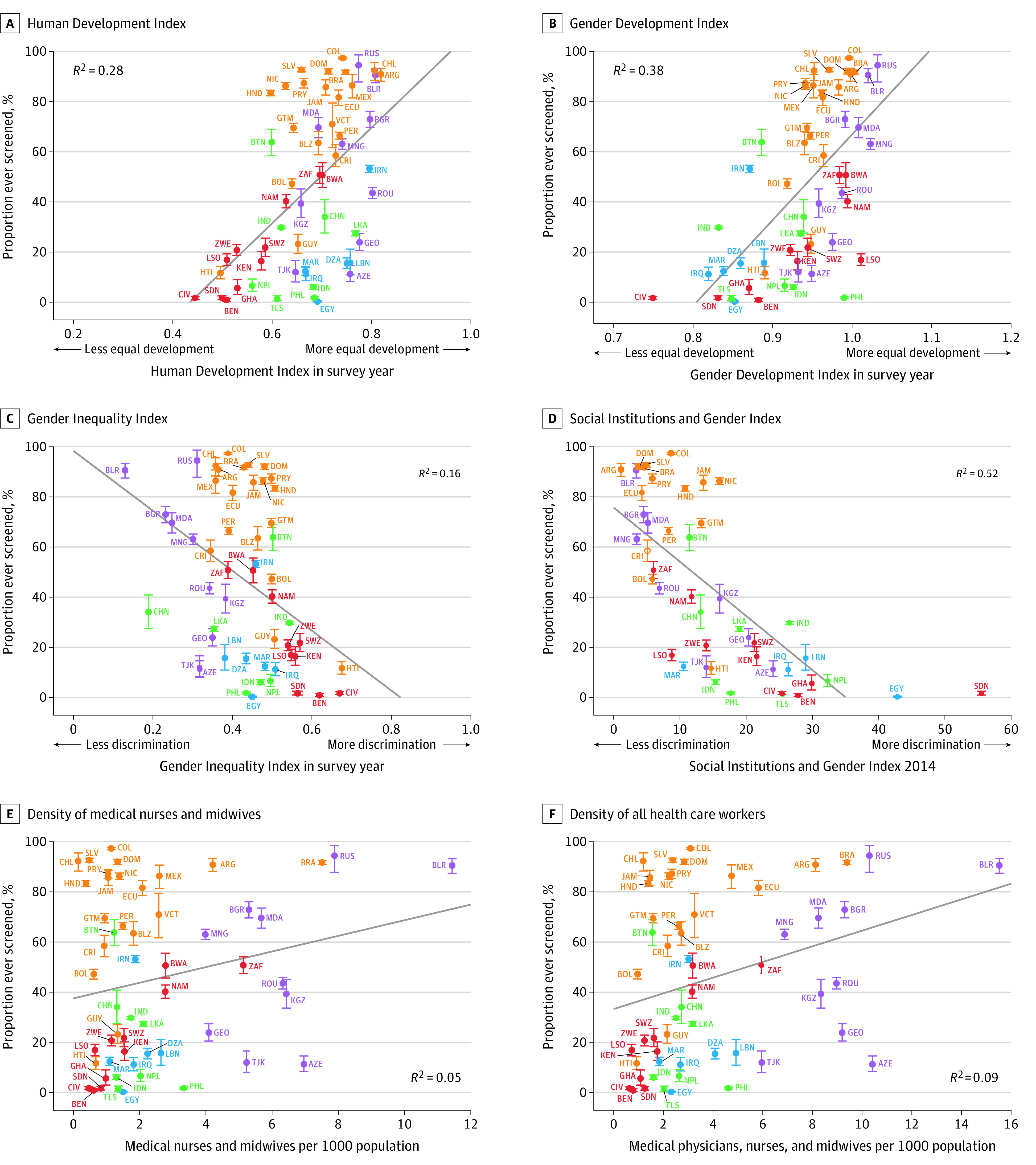
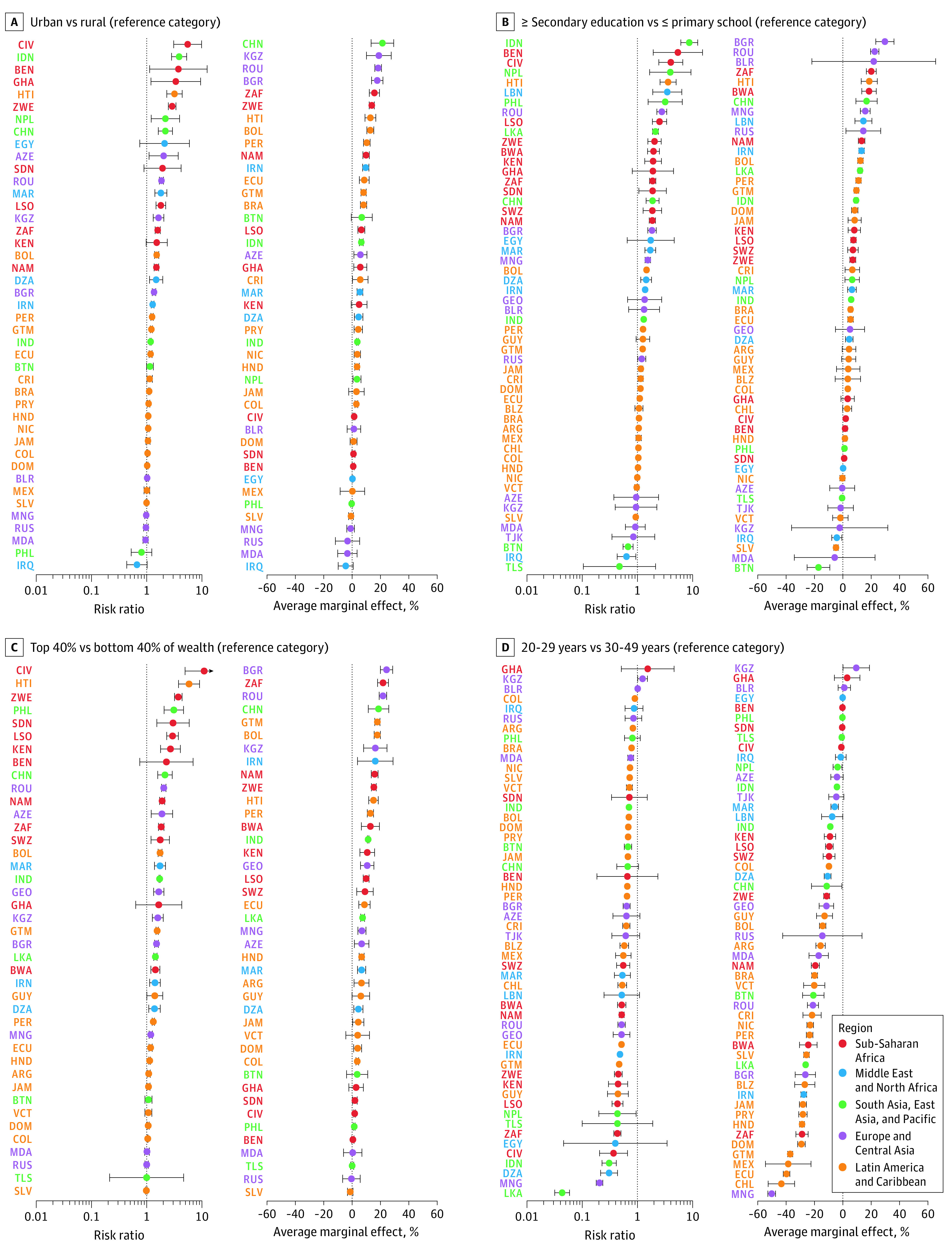
Results: Of the 1 129 404 women included in the analysis, 542 475 were aged 30 through 49 years. A country-level median of 43.6% (interquartile range [IQR], 13.9%-77.3%; range, 0.3%-97.4%) of women aged 30 through 49 years self-reported to have ever been screened, with countries in Latin America and the Caribbean having the highest prevalence (country-level median, 84.6%; IQR, 65.7%-91.1%; range, 11.7%-97.4%) and those in sub-Saharan Africa the lowest prevalence (country-level median, 16.9%; IQR, 3.7%-31.0%; range, 0.9%-50.8%). There was large variation in the self-reported lifetime prevalence of cervical cancer screening among countries within regions and among countries with similar levels of per capita gross domestic product and total health expenditure. Within countries, women who lived in rural areas, had low educational attainment, or had low household wealth were generally least likely to self-report ever having been screened.
Conclusions and relevance: In this cross-sectional study of data collected in 55 low- and middle-income countries from 2005 through 2018, there was wide variation between countries in the self-reported lifetime prevalence of cervical cancer screening. However, the median prevalence was only 44%, supporting the need to increase the rate of screening.
Conflict of interest statement
Figures
Comment in
-
Cervical Cancer Screening in Low- and Middle-Income Countries.JAMA. 2021 Feb 23;325(8):790. doi: 10.1001/jama.2020.25214. JAMA. 2021. PMID: 33620396 No abstract available.
