

Changes in Cigarette Consumption With Reduced Nicotine Content Cigarettes Among Smokers With Psychiatric Conditions or Socioeconomic Disadvantage: 3 Randomized Clinical Trials
- PMID: 33079196
- PMCID: PMC7576411
- DOI: 10.1001/jamanetworkopen.2020.19311
Changes in Cigarette Consumption With Reduced Nicotine Content Cigarettes Among Smokers With Psychiatric Conditions or Socioeconomic Disadvantage: 3 Randomized Clinical Trials
Abstract
Importance: This study is part of a programmatic effort evaluating the effects of reducing nicotine content of cigarettes to minimally addictive levels.
Objective: To examine whether very low-nicotine-content (VLNC) cigarettes decrease smoking rates and dependence severity among smokers with psychiatric disorders or socioeconomic disadvantage.
Design, setting, and participants: These 3 randomized clinical trials were performed at the University of Vermont, Brown University, and Johns Hopkins University between October 2016 and September 2019. Participants received 12 weeks of exposure to study cigarettes with nicotine content ranging from levels representative of commercial cigarettes (15.8 mg nicotine/g tobacco) to less than a hypothesized addiction threshold (2.4 mg/g and 0.4 mg/g). Daily smokers from 3 at-risk populations participated: individuals with affective disorders, exemplifying smokers with mental illness; individuals with opioid use disorder, exemplifying smokers with substance use disorders; and women with high school educations or less, exemplifying smokers with socioeconomic disadvantage. Data were analyzed from September 2019 to July 2020.
Interventions: Random assignment to 1 of 3 study cigarettes provided weekly at no cost for 12 weeks.
Main outcomes and measures: The primary outcome was between-group differences in mean total cigarettes smoked daily (CPD) during week 12; secondary outcomes included CPD for study and nonstudy cigarettes and dependence severity across weeks analyzed using analysis of covariance, random coefficients growth modeling, or repeated measures analysis of variance.
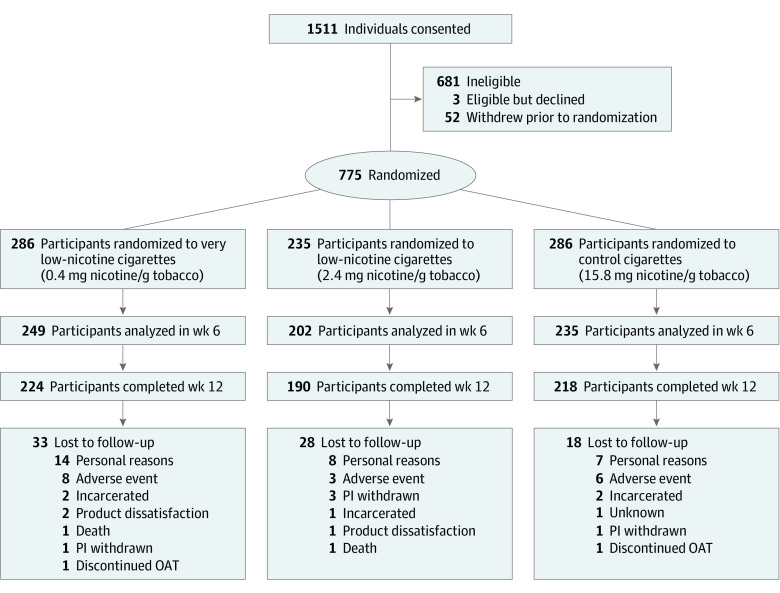
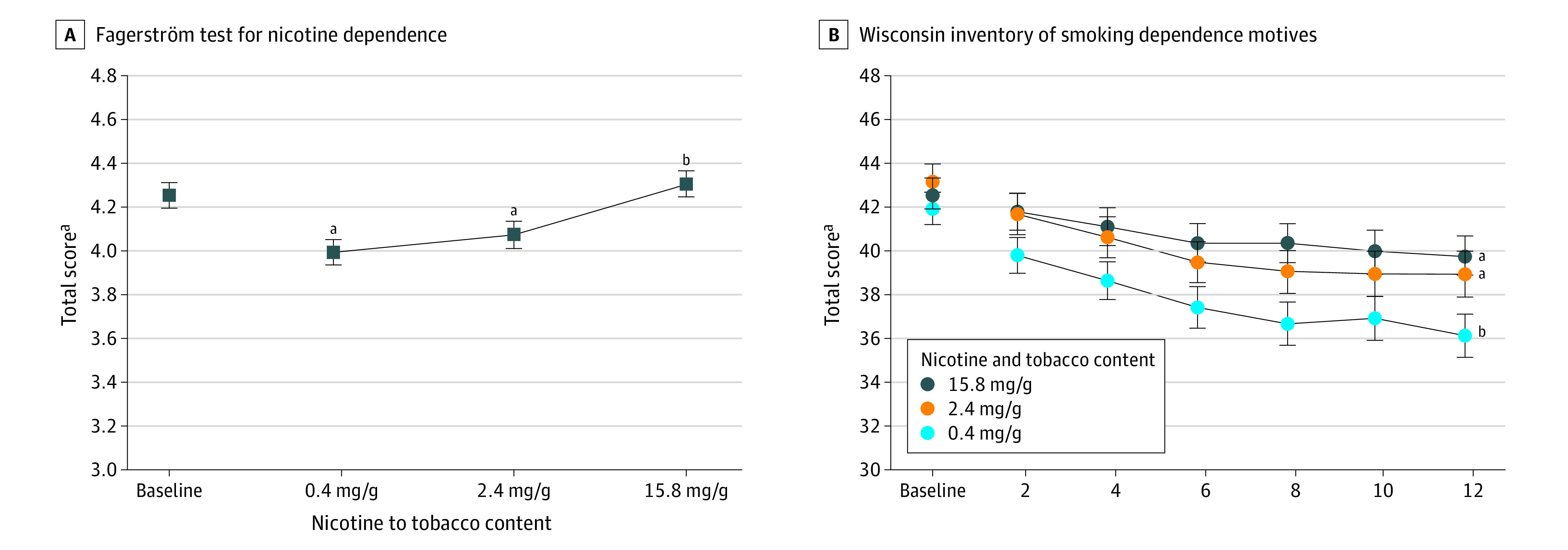
Results: A total of 775 participants were included (mean [SD] age, 35.59 [11.05] years; 551 [71.10%] women [owing to 1 population being exclusively women]); participants smoked a mean (SD) of 17.79 (9.18) CPD at study intake. A total of 286 participants were randomized to 0.4 mg/g, 235 participants were randomized to 2.4 mg/g, and 254 participants were randomized to 15.8 mg/g. Participants randomized to VLNC cigarettes had decreased mean [SEM] total CPD during week 12 across populations (Cohen d = 0.61; P < .001). At week 12, mean (SEM) CPD decreased to 17.96 (0.98) CPD in the 0.4 mg/g group and to 19.53 (1.07) CPD in the 2.4 mg/g group, both of which were significantly different from the 15.8 mg/g group (25.08 [1.08] CPD at week 12) but not each other (0.4 mg/g adjusted mean difference: -7.54 [95%CI, -9.51 to -5.57]; 2.4 mg/g adjusted mean difference: -5.34 [95% CI, 7.41 to -3.26]). Several secondary outcomes differed across populations randomized to VLNCs, including mean total CPD across weeks, with linear trends lower in participants receiving 0.4 mg/g (-0.28 [95%CI, -0.39 to -0.18]; P < .001) and 2.4 mg/g (-0.13 [95%CI, -0.25 to -0.01]; P < .001) doses compared with those receiving the 15.8 mg/g dose (0.30 [95% CI, 0.19 to 0.41]). Fagerström Test of Nicotine Dependence mean total scores were significantly lower in participants who received VLNCs (Cohen d = 0.12; P < .001), with those who received the 0.4 mg/g dose (mean [SD] score, 3.99 [0.06]; P < .001 vs 15.8 mg/g) or 2.4 mg/g dose (mean [SD] score, 4.07 [0.06]; P = .01 vs 15.8 mg/g) differing from those who received the 15.8 mg/g dose (mean [SD] score, 4.31 [0.06]) but not from each other.
Conclusions and relevance: These findings demonstrate that decreasing the nicotine content of cigarettes to very low levels reduced smoking rate and nicotine-dependence severity in these high-risk populations, effects that may facilitate successful cessation.
Trial registration: ClinicalTrials.gov Identifiers: NCT02232737, NCT02250664, NCT02250534.
Conflict of interest statement
Figures

Comment in
-
Is Nicotine Reduction in Cigarettes Enough?JAMA Netw Open. 2020 Oct 1;3(10):e2019367. doi: 10.1001/jamanetworkopen.2020.19367. JAMA Netw Open. 2020. PMID: 33079192 No abstract available.
References
-
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Centers for Disease Control and Prevention; 2014. - PubMed
