

Sepsis and septic shock in France: incidences, outcomes and costs of care
- PMID: 33079281
- PMCID: PMC7575668
- DOI: 10.1186/s13613-020-00760-x
Sepsis and septic shock in France: incidences, outcomes and costs of care
Abstract
Background: Sepsis is one of the leading causes of death worldwide. The associated incidence, mortality and trends do not differ greatly between documented reports. The purpose of this study was to provide an in-depth description of patients with sepsis and septic shock hospitalized in France from 2010 to 2015 and to explore the temporal trends of their clinical characteristics, costs and outcomes.
Methods: Retrospective cohort study of the French hospital administrative database in which organ failure therapies and severity scores are systematically registered. All patients admitted between 2010 and 2015 for sepsis and septic shock as defined by an ICD-10 code for infection, and for organ failure or the use of organ failure supplementation were included. Incidence, outcomes and trends were analyzed. Subgroup analyses based on several coding strategies and adjusted for severity scores were performed.
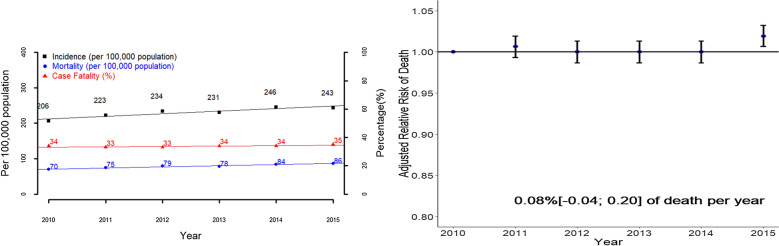
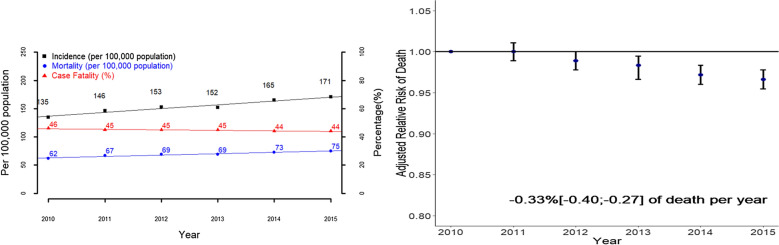
Results: A total of 737,147 patients with sepsis and 492,902 patients with septic shock were included. From 2010 to 2015, the incidence of sepsis and septic shock increased, respectively, from 206 to 243 and from 135 to 171 cases per 100,000 population. Case fatality remained at 34% for sepsis, but decreased from 46 to 44% for septic shock. Median hospital stay costs amounted to €11,400 (IQR: 5036; 24,364) for patients with sepsis and €16,439 (IQR: 7339; 29,360) for patients with septic shock. After adjustment for case-mix and illness severity, the risk of death was stable for sepsis (0.08% [- 0.04; 0.20] per year), but decreased for sepsis patients admitted to the intensive care unit and for cases of septic shock (- 0.33%[ - 0.40; - 0.27] per year).
Conclusions: Sepsis is common, frequently fatal and expensive to treat. Its incidence has increased. Case fatality has decreased in most severely affected patients, owing partly to general improvements in care.
Keywords: Epidemiology; Secular trends; Sepsis; Septic shock.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
