

Use of Higher-strength Opioids has a Dose-Dependent Association With Reoperations After Lumbar Decompression and Interbody Fusion Surgery
- PMID: 33079910
- PMCID: PMC11296383
- DOI: 10.1097/BRS.0000000000003751
Use of Higher-strength Opioids has a Dose-Dependent Association With Reoperations After Lumbar Decompression and Interbody Fusion Surgery
Abstract
Study design: A retrospective cohort study.
Objective: The aim of this study was to identify an association between preoperative opioid use and reoperations rates.
Summary of background data: Chronic opioid use is a public health crisis in the United States and has been linked to worse outcomes after lumbar spine surgery. However, no studies have identified an association between preoperative opioid use and reoperations rates.
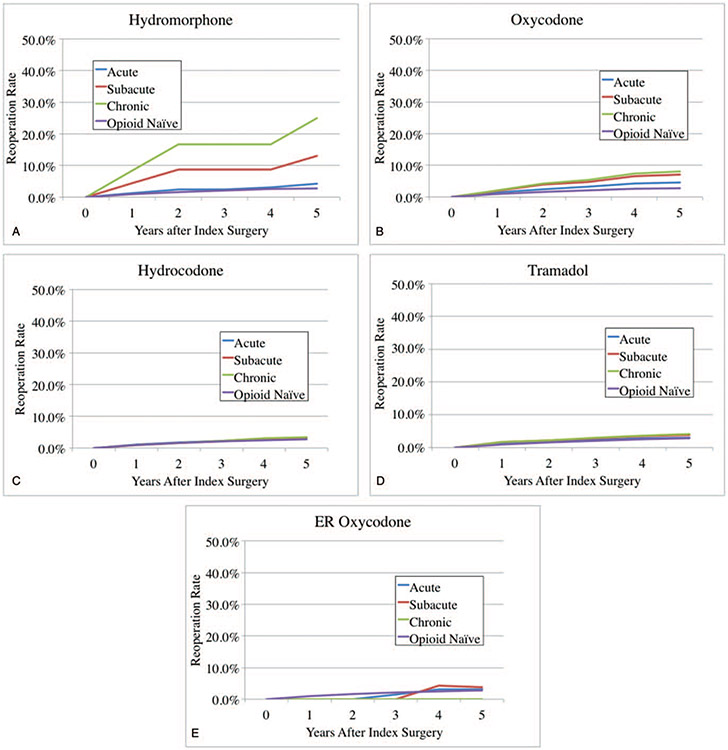
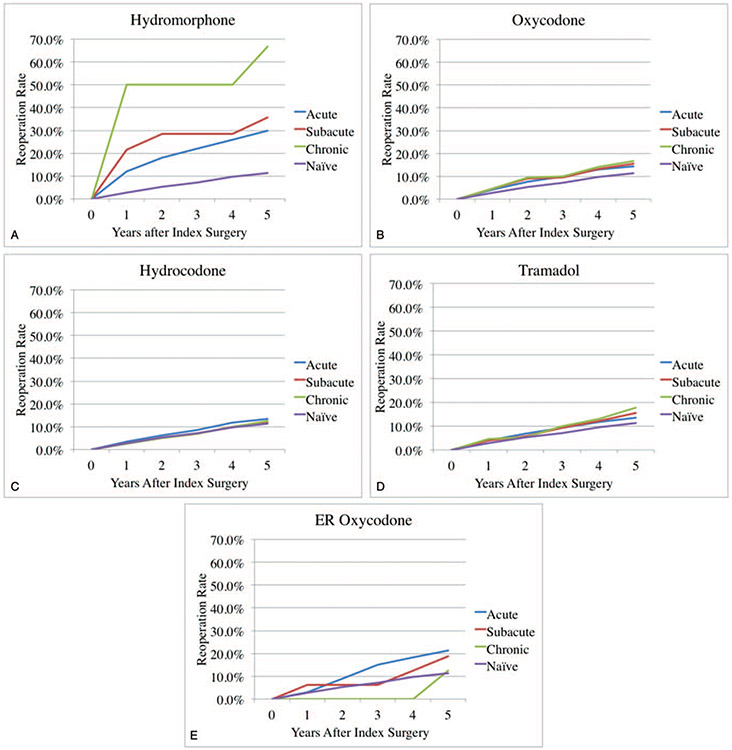
Methods: A retrospective cohort study was conducted using patients from one private insurance database who underwent primary lumbar decompression/discectomy (LDD) or posterior/transforaminal lumbar interbody fusion (PLIF/TLIF). Preoperative use of five specific opioid medications (tramadol, hydromorphone, oxycodone, hydromorphone, and extended-release oxycodone) was categorized as acute (within 3 months), subacute (acute use and use between 3 and 6 months), or chronic (subacute use and use before 6 months). Multivariate regression, controlling for multilevel surgery, age, sex, and Charlson Comorbidity Index, was used to determine the association of each medication on reoperations within 5 years.
Results: A total of 11,551 patients undergoing LDD and 3291 patients undergoing PLIF/TLIF without previous lumbar spine surgery were identified. In the LDD group, opioid-naïve patients had a 5-year reoperation rate of 2.8%, compared with 25.0% and 8.0 with chronic preoperative use of hydromorphone and oxycodone, respectively. In multivariate analysis, any preoperative use of oxycodone was associated with increased reoperations (odds ratios [OR] = 1.4, 2.0, and 2.3, for acute, subacute, and chronic use; P < 0.01). Chronic use of hydromorphone was also associated with increased reoperations (OR = 7.5, P < 0.01).In the PLIF/TLIF group, opioid-naïve patients had a 5-year reoperation rate of 11.3%, compared with 66.7% and 16.8% with chronic preoperative use of hydromorphone and oxycodone, respectively. In multivariate analysis, any preoperative use of hydromorphone was associated with increased reoperations (OR = 2.9, 4.0, and 14.0, for acute, subacute, and chronic use; P < 0.05).
Conclusion: Preoperative use of the higher-potency opioid medications is associated with increased reoperations after LDD and PLIF/TLIF in a dose-dependent manner. Surgeons should use this data for preoperative opioid cessation counseling and individualized risk stratification.Level of Evidence: 3.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Figures
Similar articles
-
Association of Duration of Preoperative Opioid Use with Reoperation After One-level Anterior Cervical Discectomy and Fusion in Nonmyelopathic Patients.Spine (Phila Pa 1976). 2021 Jul 1;46(13):E719-E725. doi: 10.1097/BRS.0000000000003861. Spine (Phila Pa 1976). 2021. PMID: 33290380
-
Preoperative opioids before adult spinal deformity surgery associated with increased reoperations and high rates of chronic postoperative opioid use at 3-year follow-up.Spine Deform. 2022 May;10(3):615-623. doi: 10.1007/s43390-021-00450-z. Epub 2022 Jan 22. Spine Deform. 2022. PMID: 35066794 Free PMC article.
-
Cost-effectiveness of posterior lumbar interbody fusion and/or transforaminal lumbar interbody fusion for grade 1 lumbar spondylolisthesis: a 5-year Quality Outcomes Database study.J Neurosurg Spine. 2024 Aug 16;41(5):596-603. doi: 10.3171/2024.5.SPINE24112. Print 2024 Nov 1. J Neurosurg Spine. 2024. PMID: 39151203
-
Comparison of (Partial) economic evaluations of transforaminal lumbar interbody fusion (TLIF) versus Posterior lumbar interbody fusion (PLIF) in adults with lumbar spondylolisthesis: A systematic review.PLoS One. 2021 Feb 11;16(2):e0245963. doi: 10.1371/journal.pone.0245963. eCollection 2021. PLoS One. 2021. PMID: 33571291 Free PMC article.
-
A perspective on reoperations after surgical treatments of degenerative lumbar diseases.J Orthop Translat. 2025 Mar 13;51:159-162. doi: 10.1016/j.jot.2025.01.014. eCollection 2025 Mar. J Orthop Translat. 2025. PMID: 40160810 Free PMC article. Review.
Cited by
-
Efficacy of Duloxetine for Postspine Surgery Pain: A Systematic Review and Meta-Analysis.Brain Behav. 2025 Jan;15(1):e70217. doi: 10.1002/brb3.70217. Brain Behav. 2025. PMID: 39740780 Free PMC article.
-
The efficacy of thoracolumbar interfascial plane block for lumbar spinal surgeries: a systematic review and meta-analysis.J Orthop Surg Res. 2023 Apr 25;18(1):318. doi: 10.1186/s13018-023-03798-2. J Orthop Surg Res. 2023. PMID: 37095532 Free PMC article.
-
Management of Postoperative Pain in Patients Following Spine Surgery: A Narrative Review.Int J Gen Med. 2022 May 2;15:4535-4549. doi: 10.2147/IJGM.S292698. eCollection 2022. Int J Gen Med. 2022. PMID: 35528286 Free PMC article. Review.
References
-
- Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med 2010;363:1981–5. - PubMed
-
- Birnbaum HG, White AG, Schiller M, et al. Societal costs of prescription opioid abuse, dependence, and misuse in the United States. Pain Med 2011;12:657–67. - PubMed
-
- Gerbershagen HJ, Aduckathil S, van Wijck AJ, et al. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013;118:934–44. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
