

Optimal time interval between hysteroscopic polypectomy and frozen-thawed blastocyst transfer: A retrospective study
- PMID: 33079974
- PMCID: PMC7575078
- DOI: 10.1371/journal.pone.0240882
Optimal time interval between hysteroscopic polypectomy and frozen-thawed blastocyst transfer: A retrospective study
Abstract
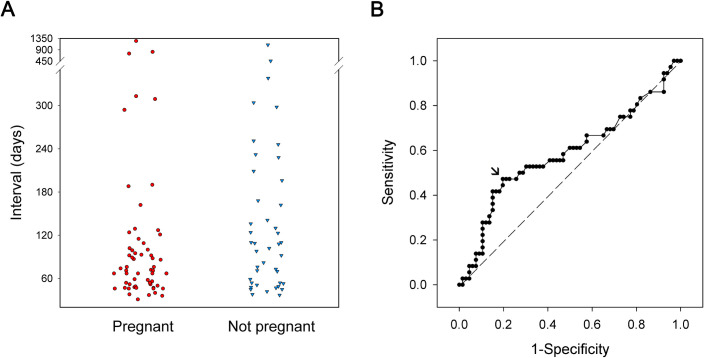
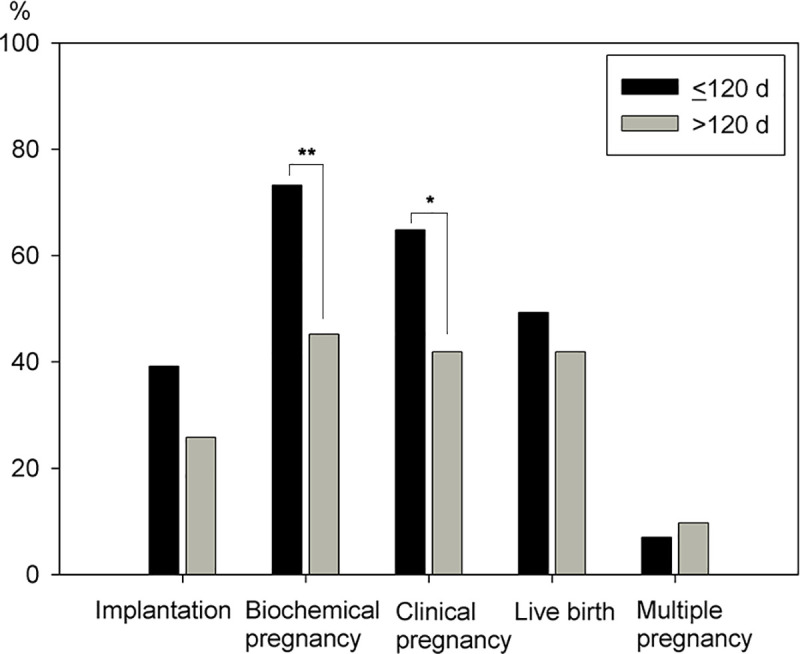
The optimal timing of frozen-thawed blastocyst transfer following hysteroscopic polypectomy is an important and unanswered clinical question. In this study, we conducted a retrospective survey of cases from an infertility center at an academic hospital. We reviewed the charts of all patients who received in-vitro fertilization and frozen-thawed blastocyst transfers (FBT) at the center from January 2009 to November 2019. One hundred and two patients with prior diagnosis of endometrial polyp that were treated with hysteroscopic polypectomy before received their first FBT at the center were identified as cases. Patients without prior diagnosis of endometrial polyp, and who received their first FBT at the center were defined as controls. Controls were enrolled at a 1-to-1 ratio to the cases. The cases and controls did not show differences in baseline characteristics, endometrial thickness, or the number of good blastocysts transferred. The clinical pregnancy rates and live birth rates were similar. Regarding the optimal interval between polypectomy and FBT, a cut-off of 120 days was identified from the ROC curve. A stratified analysis showed that when FBT was performed within an interval of 120 days after polypectomy, there were higher biochemical pregnancy rates (73.2%, 45.2%; OR 3.3; P = .007) and clinical pregnancy rates (64.8%, 41.9%; OR 2.54; P = .032), when compared with intervals greater than 120 days. There were no significant differences in implantation and live birth rates. In conclusion, pregnancy rates following FBT in patients who had received prior endometrial polypectomy were comparable to pregnancy rates after FBT in patients without endometrial polyp. Subgroup analysis showed that an interval greater than 120 days between hysteroscopic polypectomy and FBT was associated with decreased pregnancy rates. Patients who wish to receive embryo transfer after polypectomy should wait no longer than 120 days.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
