

Differential immunological signature at the culprit site distinguishes acute coronary syndrome with intact from acute coronary syndrome with ruptured fibrous cap: results from the prospective translational OPTICO-ACS study
- PMID: 33080003
- PMCID: PMC7780480
- DOI: 10.1093/eurheartj/ehaa703
Differential immunological signature at the culprit site distinguishes acute coronary syndrome with intact from acute coronary syndrome with ruptured fibrous cap: results from the prospective translational OPTICO-ACS study
Abstract
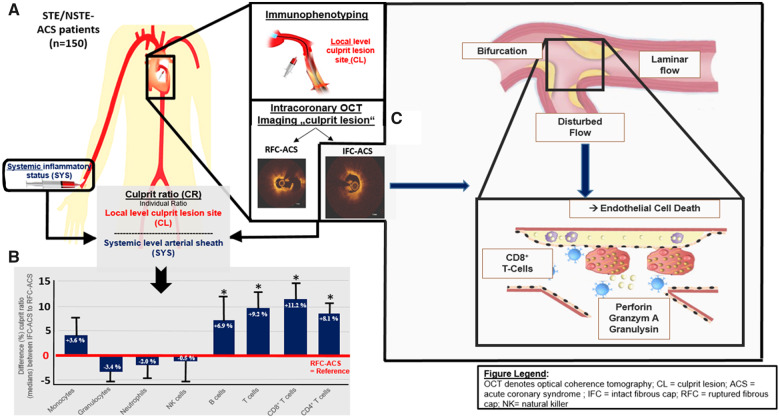
Aims: Acute coronary syndromes with intact fibrous cap (IFC-ACS), i.e. caused by coronary plaque erosion, account for approximately one-third of ACS. However, the underlying pathophysiological mechanisms as compared with ACS caused by plaque rupture (RFC-ACS) remain largely undefined. The prospective translational OPTICO-ACS study programme investigates for the first time the microenvironment of ACS-causing culprit lesions (CL) with intact fibrous cap by molecular high-resolution intracoronary imaging and simultaneous local immunological phenotyping.
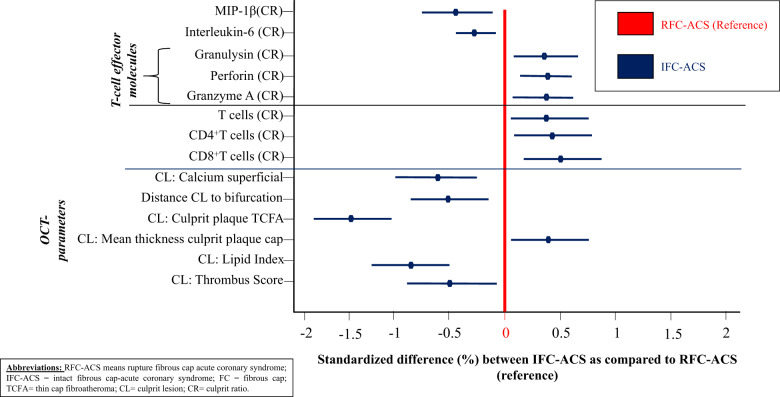
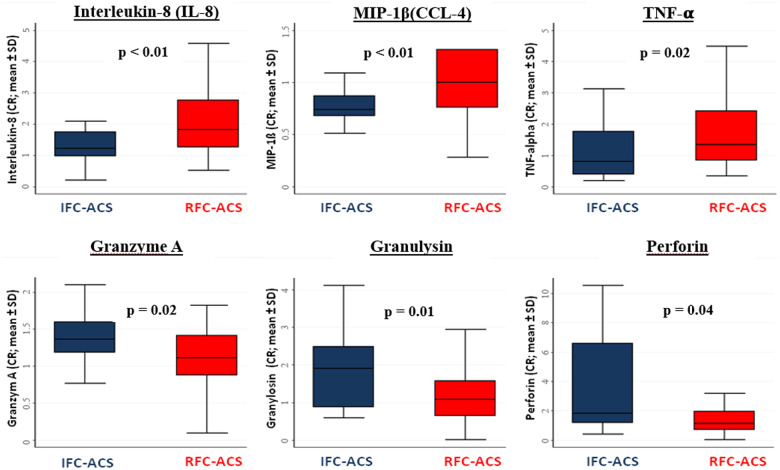
Methods and results: The CL of 170 consecutive ACS patients were investigated by optical coherence tomography (OCT) and simultaneous immunophenotyping by flow cytometric analysis as well as by effector molecule concentration measurements across the culprit lesion gradient (ratio local/systemic levels). Within the study cohort, IFC caused 24.6% of ACS while RFC-ACS caused 75.4% as determined and validated by two independent OCT core laboratories. The IFC-CL were characterized by lower lipid content, less calcification, a thicker overlying fibrous cap, and largely localized near a coronary bifurcation as compared with RFC-CL. The microenvironment of IFC-ACS lesions demonstrated selective enrichment in both CD4+ and CD8+ T-lymphocytes (+8.1% and +11.2%, respectively, both P < 0.05) as compared with RFC-ACS lesions. T-cell-associated extracellular circulating microvesicles (MV) were more pronounced in IFC-ACS lesions and a significantly higher amount of CD8+ T-lymphocytes was detectable in thrombi aspirated from IFC-culprit sites. Furthermore, IFC-ACS lesions showed increased levels of the T-cell effector molecules granzyme A (+22.4%), perforin (+58.8%), and granulysin (+75.4%) as compared with RFC plaques (P < 0.005). Endothelial cells subjected to culture in disturbed laminar flow conditions, i.e. to simulate coronary flow near a bifurcation, demonstrated an enhanced adhesion of CD8+T cells. Finally, both CD8+T cells and their cytotoxic effector molecules caused endothelial cell death, a key potential pathophysiological mechanism in IFC-ACS.
Conclusions: The OPTICO-ACS study emphasizes a novel mechanism in the pathogenesis of IFC-ACS, favouring participation of the adaptive immune system, particularly CD4+ and CD8+ T-cells and their effector molecules. The different immune signatures identified in this study advance the understanding of coronary plaque progression and may provide a basis for future development of personalized therapeutic approaches to ACS with IFC.
Trial registration: The study was registered at clinicalTrials.gov (NCT03129503).
Keywords: Acute coronary syndrome; CD8+; Endothelial erosion; Optical coherence tomography; Plaque rupture; Shear stress; T cells.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures

Comment in
-
CD8 lymphocytes and plaque erosion: a new piece in the jigsaw.Eur Heart J. 2020 Oct 1;41(37):3561-3563. doi: 10.1093/eurheartj/ehaa721. Eur Heart J. 2020. PMID: 33079982 No abstract available.
References
-
- Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM.. Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–1275. - PubMed
-
- Bentzon JF, Otsuka F, Virmani R, Falk E.. Mechanisms of plaque formation and rupture. Circ Res 2014;114:1852–1866. - PubMed
-
- Fujii K, Kawasaki D, Masutani M, Okumura T, Akagami T, Sakoda T, Tsujino T, Ohyanagi M, Masuyama T.. OCT assessment of thin-cap fibroatheroma distribution in native coronary arteries. JACC Cardiovasc Imaging 2010;3:168–175. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
