

Rectal nonsteroidal anti-inflammatory drugs and pancreatic stents in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis in high-risk patients: A network meta-analysis
- PMID: 33080710
- PMCID: PMC7571888
- DOI: 10.1097/MD.0000000000022672
Rectal nonsteroidal anti-inflammatory drugs and pancreatic stents in preventing post-endoscopic retrograde cholangiopancreatography pancreatitis in high-risk patients: A network meta-analysis
Abstract
Background: 100 mg rectal nonsteroidal anti-inflammatory drugs (NSAIDs) and pancreatic stents both significantly reduce the incidence of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis. Direct comparison of randomized controlled trials (RCTs) between them in high-risk patients is absent. We conducted this network meta-analysis to indirectly compare the efficacies of 100 mg rectal NSAIDs and pancreatic stents in preventing post-ERCP pancreatitis (PEP) in high-risk patients and help us decide which is preferred in clinical practice.
Methods: A comprehensive search was done to identify RCTs published in English full-text. Interventions included 100 mg rectal NSAIDs (diclofenac or indomethacin) and pancreatic stents. Only studies with high-risk patients of PEP were included. Meta-analyses of NSAIDs and pancreatic stents were conducted respectively. A network meta-analysis using the Bayesian method was performed.
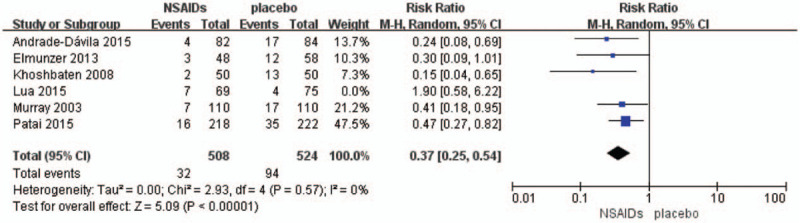
Results: We included 14 RCTs, 8 on pancreatic stents and 6 on 100 mg rectal NSAIDs in high-risk patients. There was no direct comparison between them. After excluding an outlier study on NSAIDs (n = 144), meta-analyses showed they both significantly and statistically reduced the incidence of PEP in high-risk patients (pancreatic stents: n = 8 studies, random-effects risk ratio (RR)0.41, 95%CI 0.30-0.56, I = 0%; NSAIDs: n = 5 studies, random-effects RR 0.37, 95%CI 0.25-0.54, I = 0%). And network meta-analysis showed efficacy of 100 mg rectal NSAIDs was equal to pancreatic stents (random-effects RR 0.94, 95%CI 0.50-1.8).
Conclusions: The efficacy of 100 mg rectal NSAIDs (diclofenac or indomethacin) seems equally significant to pancreatic stents in preventing PEP in high-risk patients. Considering the cost-effectiveness and safety, 100 mg diclofenac or indomethacin may be preferred.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures








Similar articles
-
Non-steroidal anti-inflammatory drugs, intravenous fluids, pancreatic stents, or their combinations for the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a systematic review and network meta-analysis.Lancet Gastroenterol Hepatol. 2021 Sep;6(9):733-742. doi: 10.1016/S2468-1253(21)00170-9. Epub 2021 Jun 30. Lancet Gastroenterol Hepatol. 2021. PMID: 34214449
-
What is impact of nonsteroidal anti-inflammatory drugs in the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a meta-analysis of randomized controlled trials.BMC Gastroenterol. 2018 Jul 4;18(1):106. doi: 10.1186/s12876-018-0837-4. BMC Gastroenterol. 2018. PMID: 29973142 Free PMC article. Review.
-
Rectal nonsteroidal anti-inflammatory drugs are superior to pancreatic duct stents in preventing pancreatitis after endoscopic retrograde cholangiopancreatography: a network meta-analysis.Clin Gastroenterol Hepatol. 2013 Jul;11(7):778-83. doi: 10.1016/j.cgh.2012.12.043. Epub 2013 Jan 30. Clin Gastroenterol Hepatol. 2013. PMID: 23376320 Review.
-
Rectal nonsteroidal anti-inflammatory drugs administration is effective for the prevention of post-ERCP pancreatitis: An updated meta-analysis of randomized controlled trials.Pancreatology. 2017 Sep-Oct;17(5):681-688. doi: 10.1016/j.pan.2017.07.008. Epub 2017 Jul 17. Pancreatology. 2017. PMID: 28734720
-
Efficacy of Combined Management with Nonsteroidal Anti-inflammatory Drugs for Prevention of Pancreatitis After Endoscopic Retrograde Cholangiography: a Bayesian Network Meta-analysis.J Gastrointest Surg. 2022 Sep;26(9):1982-1997. doi: 10.1007/s11605-022-05352-7. Epub 2022 Jun 9. J Gastrointest Surg. 2022. PMID: 35680777 Review.
Cited by
-
Rectal NSAIDs-based combination modalities are superior to single modalities for prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a network meta-analysis.Korean J Intern Med. 2022 Mar;37(2):322-339. doi: 10.3904/kjim.2021.410. Epub 2022 Feb 16. Korean J Intern Med. 2022. PMID: 35168302 Free PMC article.
-
A network meta-analysis of optimal strategies for preventing post-endoscopic retrograde cholangiopancreatography pancreatitis.Sci Rep. 2025 Apr 21;15(1):13702. doi: 10.1038/s41598-025-98969-y. Sci Rep. 2025. PMID: 40258999 Free PMC article.
-
Combinatorial Effect of Prophylactic Interventions for Post-ERCP Pancreatitis among Patients with Risk Factors: A Network Meta-Analysis.Gut Liver. 2023 Sep 15;17(5):814-824. doi: 10.5009/gnl220268. Epub 2022 Dec 13. Gut Liver. 2023. PMID: 36510779 Free PMC article.
-
Controversies in ERCP: Indications and preparation.Endosc Ultrasound. 2022 May-Jun;11(3):186-200. doi: 10.4103/EUS-D-21-00106. Endosc Ultrasound. 2022. PMID: 34677145 Free PMC article.
References
-
- Dumonceau JM, Kapral C, Aabakken L, et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020;52:127–49. - PubMed
-
- Pan XP, Dang T, Meng XM, et al. Clinical study on the prevention of post-ERCP pancreatitis by pancreatic duct stenting. Cell Biochem Biophys 2011;61:473–9. - PubMed
-
- Sotoudehmanesh R, Ali-Asgari A, Khatibian M, et al. Pharmacological prophylaxis versus pancreatic duct stenting plus pharmacological prophylaxis for prevention of post-ERCP pancreatitis in high risk patients: a randomized trial. Endoscopy 2019;51:915–21. - PubMed
-
- Siddiqui AA, Patel D, Kaplan J, et al. A trial of rectal indomethacin to prevent post-ercp pancreatitis in patients with suspected type 3 sphincter of oddi dysfunction. Dig Dis Sci 2015;60:2509–15. - PubMed
-
- Lang GD, Fejleh P, Bhat T, et al. No added benefit of indomethacin in the prevention of post-ercp pancreatitis after protective pancreatic duct stent placement in low risk patients. Gastrointest Endosc 2016;83:AB248.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
