

Impact of Acoustic and Interactive Disruptive Factors during Robot-Assisted Surgery-A Virtual Surgical Training Model
- PMID: 33080919
- PMCID: PMC7594064
- DOI: 10.3390/s20205891
Impact of Acoustic and Interactive Disruptive Factors during Robot-Assisted Surgery-A Virtual Surgical Training Model
Abstract
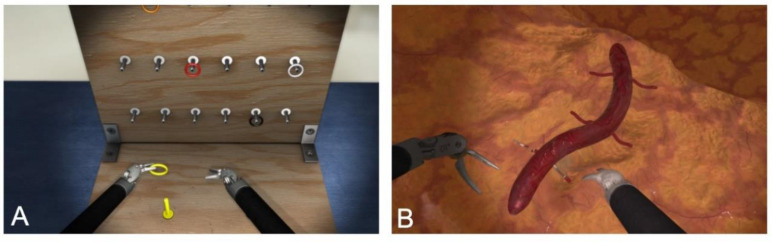
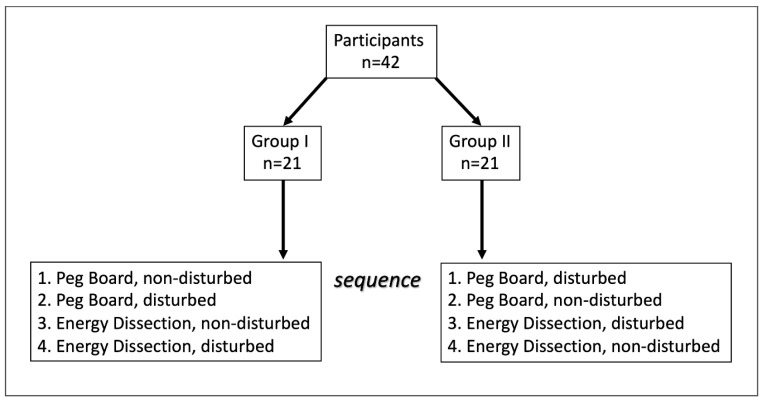
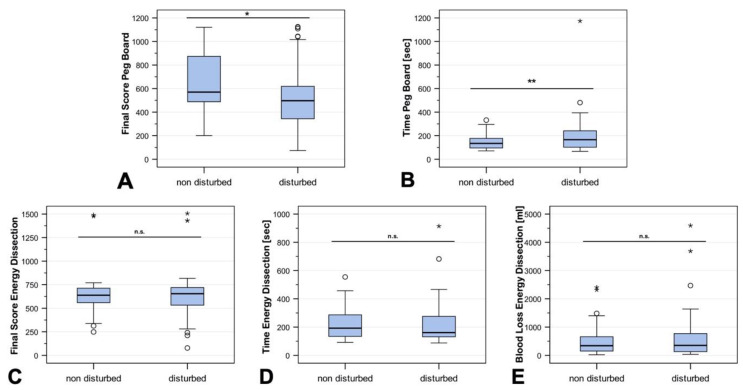
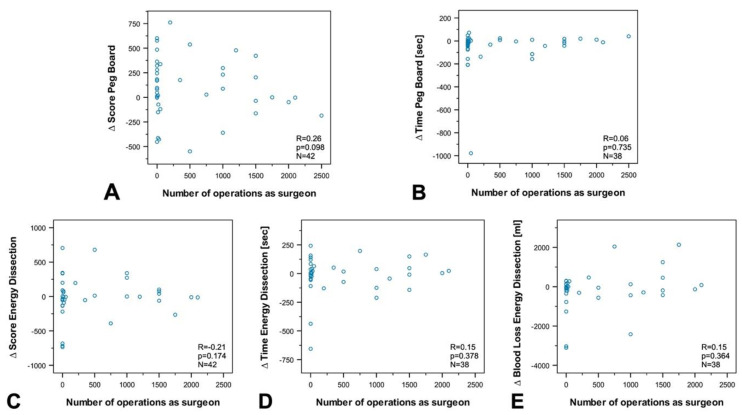
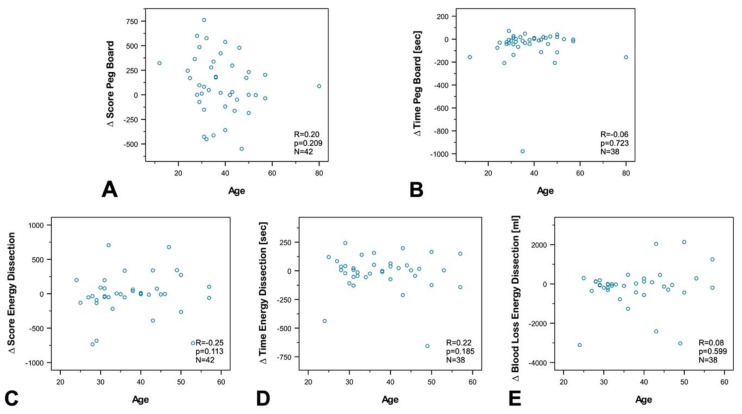
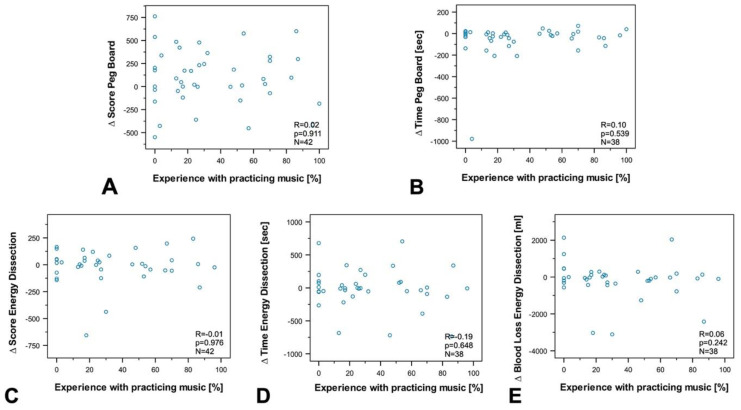
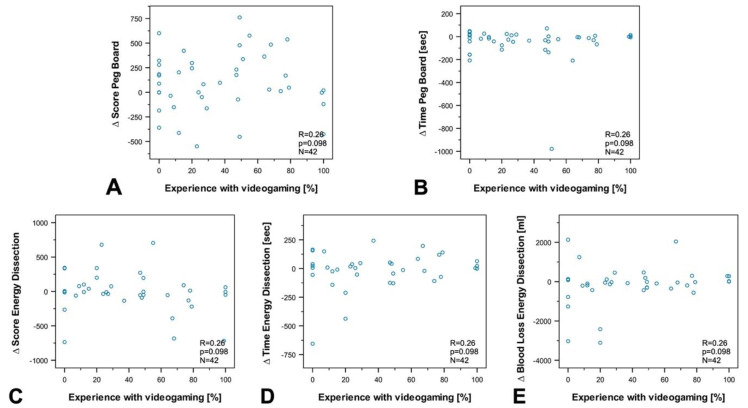
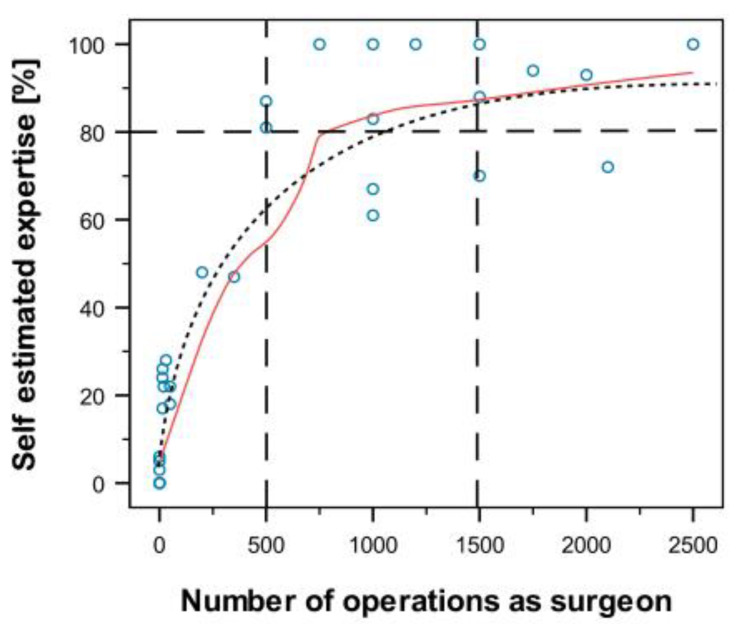
The use of virtual reality trainers for teaching minimally invasive surgical techniques has been established for a long time in conventional laparoscopy as well as robotic surgery. The aim of the present study was to evaluate the impact of reproducible disruptive factors on the surgeon's work. In a cross-sectional investigation, surgeons were tested with regard to the impact of different disruptive factors when doing exercises on a robotic-surgery simulator (Mimic Flex VRTM). Additionally, we collected data about the participants' professional experience, gender, age, expertise in playing an instrument, and expertise in playing video games. The data were collected during DRUS 2019 (Symposium of the German Society for Robot-assisted Urology). Forty-two surgeons attending DRUS 2019 were asked to participate in a virtual robotic stress training unit. The surgeons worked in various specialties (visceral surgery, gynecology, and urology) and had different levels of expertise. The time taken to complete the exercise (TTCE), the final score (FSC), and blood loss (BL) were measured. In the basic exercise with an interactive disruption, TTCE was significantly longer (p < 0.01) and FSC significantly lower (p < 0.05). No significant difference in TTCE, FSC, or BL was noted in the advanced exercise with acoustic disruption. Performance during disruption was not dependent on the level of surgical experience, gender, age, expertise in playing an instrument, or playing video games. A positive correlation was registered between self-estimation and surgical experience. Interactive disruptions have a greater impact on the performance of a surgeon than acoustic ones. Disruption affects the performance of experienced as well as inexperienced surgeons. Disruption in daily surgery should be evaluated and minimized in the interest of the patient's safety.
Keywords: complications; disruption during surgery; laparoscopy; robotic surgery; surgical education; virtual reality trainer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
A Comparison of Robotic Simulation Performance on Basic Virtual Reality Skills: Simulator Subjective Versus Objective Assessment Tools.J Minim Invasive Gynecol. 2017 Nov-Dec;24(7):1184-1189. doi: 10.1016/j.jmig.2017.07.019. Epub 2017 Jul 27. J Minim Invasive Gynecol. 2017. PMID: 28757439 Clinical Trial.
-
Outcomes of a virtual-reality simulator-training programme on basic surgical skills in robot-assisted laparoscopic surgery.Int J Med Robot. 2017 Jun;13(2). doi: 10.1002/rcs.1740. Epub 2016 Mar 1. Int J Med Robot. 2017. PMID: 26928974
-
Influence of Distraction Factors on Performance in Laparoscopic Surgery in Immersive Virtual Reality: Study Protocol of a Cross-Over Trial in Medical Students and Residents-DisLapVR.JMIR Res Protoc. 2024 Nov 5;13:e59014. doi: 10.2196/59014. JMIR Res Protoc. 2024. PMID: 39500487 Free PMC article.
-
[Methods for training of robot-assisted radical prostatectomy].Khirurgiia (Mosk). 2019;(1):89-94. doi: 10.17116/hirurgia201901189. Khirurgiia (Mosk). 2019. PMID: 30789615 Review. Russian.
-
Current state of virtual reality simulation in robotic surgery training: a review.Surg Endosc. 2016 Jun;30(6):2169-78. doi: 10.1007/s00464-015-4517-y. Epub 2015 Aug 25. Surg Endosc. 2016. PMID: 26304107 Review.
Cited by
-
Virtual reality (VR) as a simulation modality for technical skills acquisition.Ann Med Surg (Lond). 2021 Oct 27;71:102945. doi: 10.1016/j.amsu.2021.102945. eCollection 2021 Nov. Ann Med Surg (Lond). 2021. PMID: 34840738 Free PMC article. Review.
-
Assistance Robotics and Sensors.Sensors (Basel). 2023 Apr 26;23(9):4286. doi: 10.3390/s23094286. Sensors (Basel). 2023. PMID: 37177490 Free PMC article.
-
Unpacking the Broad Landscape of Intraoperative Stressors for Clinical Personnel: A Mixed-Methods Systematic Review.J Multidiscip Healthc. 2023 Jul 17;16:1953-1977. doi: 10.2147/JMDH.S401325. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37484819 Free PMC article. Review.
-
Evaluation of Laparoscopy Virtual Reality Training on the Improvement of Trainees' Surgical Skills.Medicina (Kaunas). 2021 Feb 2;57(2):130. doi: 10.3390/medicina57020130. Medicina (Kaunas). 2021. PMID: 33540817 Free PMC article.
References
-
- Elessawy M., Skrzipczyk M., Eckmann-Scholz C., Maass N., Mettler L., Guenther V., van Mackelenbergh M., Bauerschlag D.O., Alkatout I. Integration and Validation of Hysteroscopy Simulation in the Surgical Training Curriculum. J. Surg. Educ. 2017;74:84–90. doi: 10.1016/j.jsurg.2016.06.007. - DOI - PubMed
-
- Spille J., Wenners A., von Hehn U., Maass N., Pecks U., Mettler L., Alkatout I. 2D Versus 3D in Laparoscopic Surgery by Beginners and Experts: A Randomized Controlled Trial on a Pelvitrainer in Objectively Graded Surgical Steps. J. Surg. Educ. 2017;74:867–877. doi: 10.1016/j.jsurg.2017.01.011. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
