

Hypertensive Cardiotoxicity in Cancer Treatment-Systematic Analysis of Adjunct, Conventional Chemotherapy, and Novel Therapies-Epidemiology, Incidence, and Pathophysiology
- PMID: 33081013
- PMCID: PMC7603211
- DOI: 10.3390/jcm9103346
Hypertensive Cardiotoxicity in Cancer Treatment-Systematic Analysis of Adjunct, Conventional Chemotherapy, and Novel Therapies-Epidemiology, Incidence, and Pathophysiology
Abstract
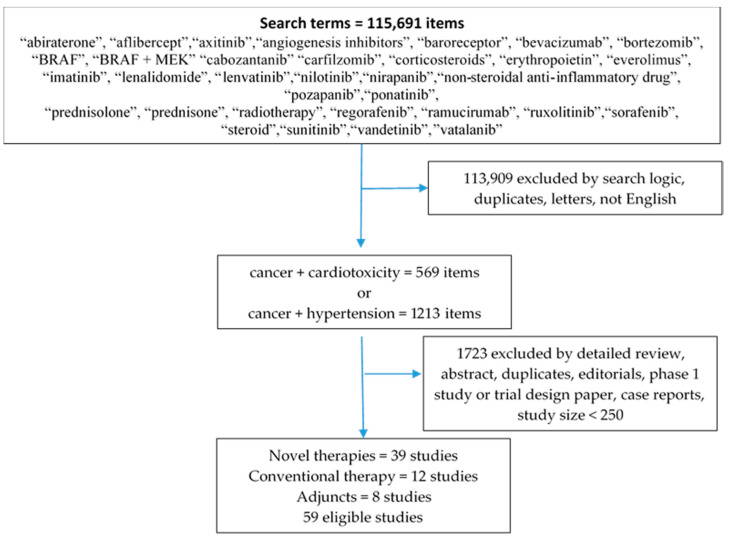
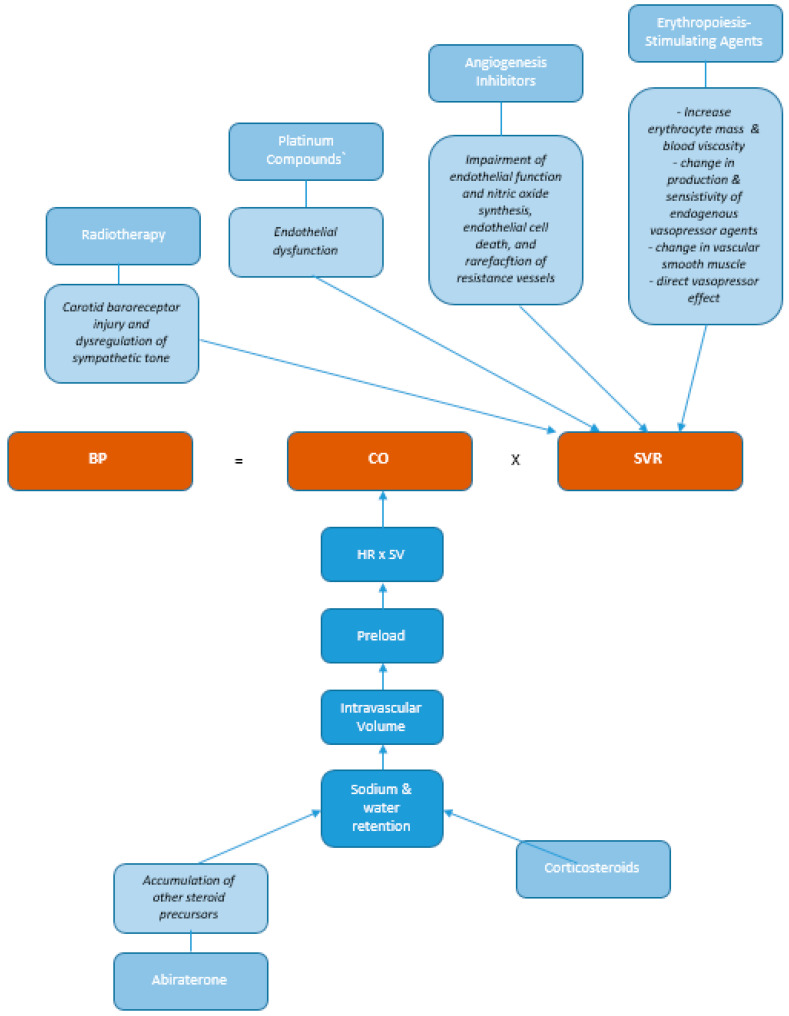
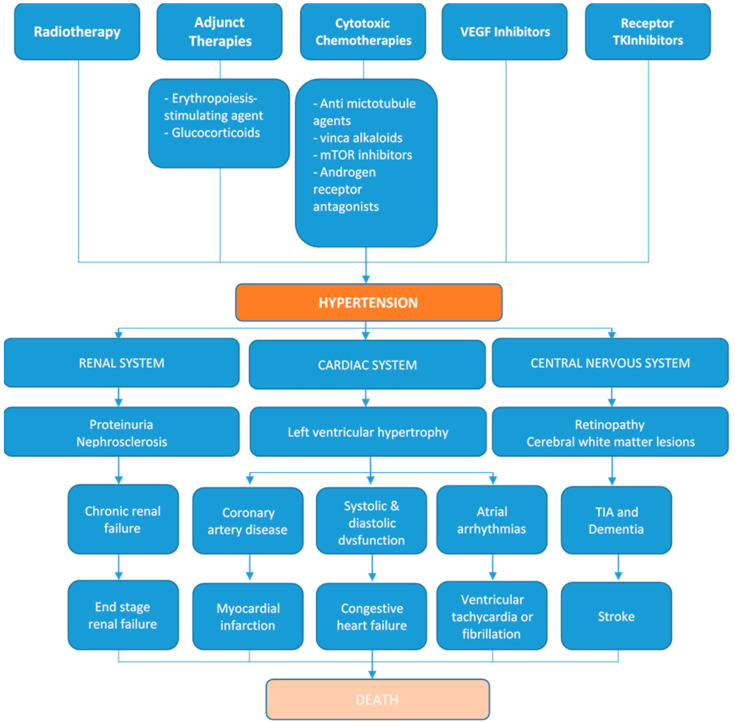
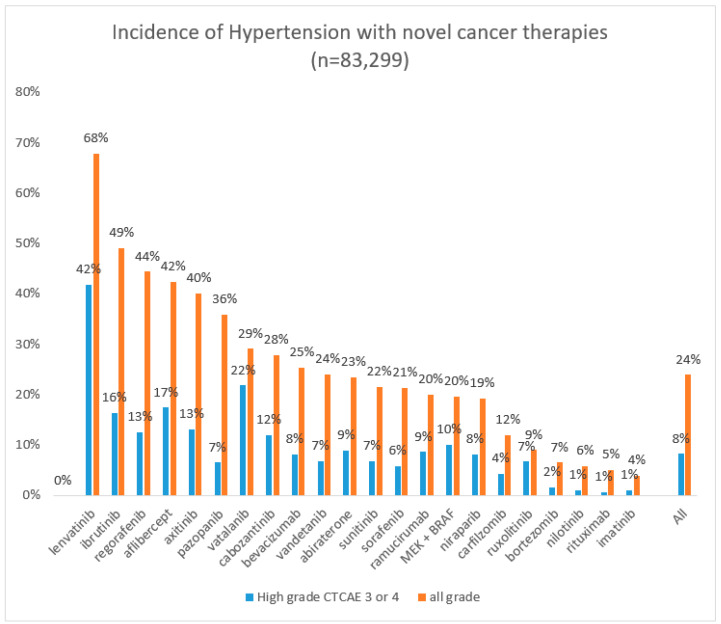
Cardiotoxicity is the umbrella term for cardiovascular side effects of cancer therapies. The most widely recognized phenotype is left ventricular dysfunction, but cardiotoxicity can manifest as arrhythmogenic, vascular, myocarditic and hypertensive toxicities. Hypertension has long been regarded as one of the most prevalent and modifiable cardiovascular risk factors in the general population, but its relevance during the cancer treatment journey may be underestimated. Hypertensive cardiotoxicity occurs de novo in a substantial proportion of treated cancer patients. The pathology is incompletely characterized-natriuresis and renin angiotensin system interactions play a role particularly in conventional treatments, but in novel therapies endothelial dysfunction and the interaction between the cancer and cardiac kinome are implicated. There exists a treatment paradox in that a significant hypertensive response not only mandates anti-hypertensive treatment, but in fact, in certain cancer treatment scenarios, hypertension is a predictor of cancer treatment efficacy and response. In this comprehensive review of over 80,000 patients, we explored the epidemiology, incidence, and mechanistic pathophysiology of hypertensive cardiotoxicity in adjunct, conventional chemotherapy, and novel cancer treatments. Conventional chemotherapy, adjunct treatments, and novel targeted therapies collectively caused new onset hypertension in 33-68% of treated patients. The incidence of hypertensive cardiotoxicity across twenty common novel therapies for any grade hypertension ranged from 4% (imatinib) to 68% (lenvatinib), and high grade 3 or 4 hypertension in < 1% (imatinib) to 42% (lenvatinib). The weighted average effect was all-grade hypertension in 24% and grade 3 or 4 hypertension in 8%.
Keywords: cancer; cardio-oncology; cardiotoxicity; hypertension; tyrosine kinase inhibitors.
Conflict of interest statement
The authors have no conflict of interests to declare.
Figures
Similar articles
-
Left Ventricular Dysfunction and Chemotherapeutic Agents.Curr Cardiol Rep. 2018 Mar 8;20(4):20. doi: 10.1007/s11886-018-0967-x. Curr Cardiol Rep. 2018. PMID: 29520629 Review.
-
Role of renin-angiotensin system antagonists in the prevention of bevacizumab- and sunitinib-mediated cardiac dysfunction.Am J Physiol Heart Circ Physiol. 2019 Mar 1;316(3):H446-H458. doi: 10.1152/ajpheart.00344.2018. Epub 2018 Nov 30. Am J Physiol Heart Circ Physiol. 2019. PMID: 30499710
-
Cardio-oncology Part I: chemotherapy and cardiovascular toxicity.Expert Rev Cardiovasc Ther. 2015 May;13(5):511-8. doi: 10.1586/14779072.2015.1032940. Epub 2015 Apr 5. Expert Rev Cardiovasc Ther. 2015. PMID: 25843285 Review.
-
Impact of Arterial Hypertension on Doxorubicin-Based Chemotherapy-Induced Subclinical Cardiac Damage in Breast Cancer Patients.Cardiovasc Toxicol. 2020 Jun;20(3):321-327. doi: 10.1007/s12012-019-09556-3. Cardiovasc Toxicol. 2020. PMID: 31782105
-
Cardiac toxicities of anticancer treatments: chemotherapy, targeted therapy and immunotherapy.Curr Opin Cardiol. 2019 Jul;34(4):441-450. doi: 10.1097/HCO.0000000000000641. Curr Opin Cardiol. 2019. PMID: 31082852 Review.
Cited by
-
Cardiac Remodeling in the Absence of Cardiac Contractile Dysfunction Is Sufficient to Promote Cancer Progression.Cells. 2022 Mar 25;11(7):1108. doi: 10.3390/cells11071108. Cells. 2022. PMID: 35406672 Free PMC article.
-
Perceptions of the Cardiologists and Oncologists: Initial Step for Establishing Cardio-Oncology Service.Front Cardiovasc Med. 2021 Nov 24;8:704029. doi: 10.3389/fcvm.2021.704029. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34917654 Free PMC article.
-
Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management.Signal Transduct Target Ther. 2023 Jul 7;8(1):262. doi: 10.1038/s41392-023-01469-6. Signal Transduct Target Ther. 2023. PMID: 37414756 Free PMC article. Review.
-
Cancer Therapy-Related Cardiovascular Complications in Clinical Practice: Current Perspectives.J Clin Med. 2021 Apr 13;10(8):1647. doi: 10.3390/jcm10081647. J Clin Med. 2021. PMID: 33924543 Free PMC article. Review.
-
Cardiovascular toxicity associated with angiogenesis inhibitors: A comprehensive pharmacovigilance analysis based on the FDA Adverse Event Reporting System database from 2014 to 2021.Front Cardiovasc Med. 2022 Oct 13;9:988013. doi: 10.3389/fcvm.2022.988013. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312283 Free PMC article.
References
-
- Beutner R. The cardiac toxicity of injectable local anesthetics. Fed. Proc. 1946;5:166. - PubMed
-
- Chapman D.W., Shaffer C.F. The mercurial diuretics; a comparison of acute cardiac toxicity in animals and the effect of ascorbic acid on detoxification in their intravenous administration. Proc. Annu. Meet. Cent. Soc. Clin. Res. US. 1946;19:7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
