

Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years-Results from the EsNuPI Study
- PMID: 33081297
- PMCID: PMC7603006
- DOI: 10.3390/nu12103171
Carbohydrates, Starch, Total Sugar, Fiber Intakes and Food Sources in Spanish Children Aged One to <10 Years-Results from the EsNuPI Study
Abstract
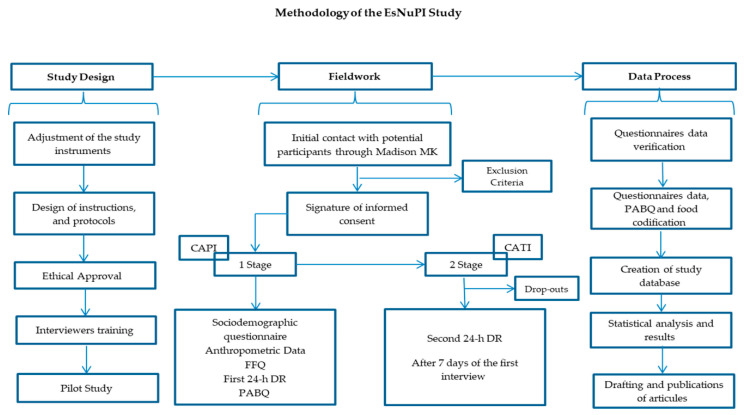
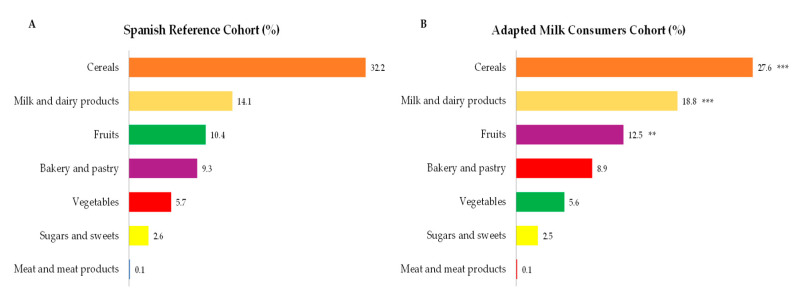
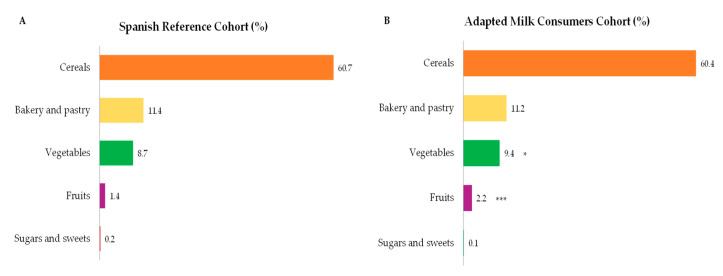
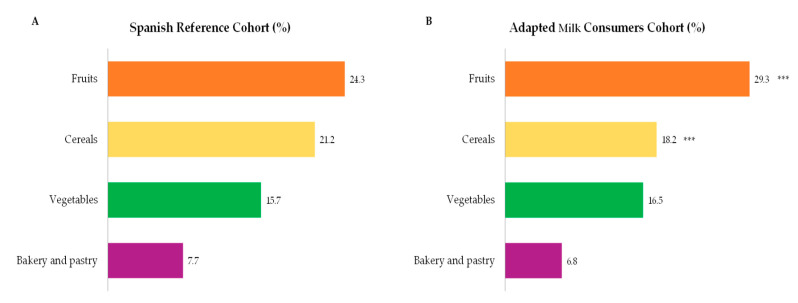
Diet quality is a modifiable factor that may contribute to the onset of diet-related chronic diseases. Currently, in Spain there are no studies that examine the intakes and sources for total carbohydrates, starch, total sugar, and fiber by both children consuming all kind of milks and children regularly consuming adapted milk formulas. Our goal was to evaluate the contribution of different food groups to total carbohydrates, starch, total sugar, and fiber consumption within the EsNuPI study participants by assessing their usual intakes by applying two 24 h dietary recalls that were completed by 1448 children (1 to <10 years) divided into two cohorts: one Spanish Reference Cohort (SRS) of the general population (n = 707) and another cohort which included children consuming adapted milks including follow-on milk, toddler's or growing up milk, fortified and enriched milks, here called Adapted Milk Consumers Cohort" (AMS) (n = 741). Estimation of the usual intake showed that nutrient intake increased with age for all nutrients except for fiber. The percentage of children by age and gender who met the reference intake (RI) range for total carbohydrates, was in all groups more than 50% of individuals, except for girls aged 6 to <10 years from the reference cohort in which only 46.9% complied the RI. Median fiber intake, both in the SRS and the AMS, was well below the adequate intake (AI) for children between 3 and 10 years. Main total carbohydrates sources were cereals, followed by milk and dairy products, fruits, bakery and pastry, vegetables and sugars and sweets. The highest contributors to starch intakes were cereals, bakery and pastry, vegetables, and fruits. Major sources of total sugar intakes were milk and dairy products, fruits, bakery and pastry, sugars and sweets, vegetables, and cereals. Nonetheless, milk and dairy products, and fruits, mainly provided lactose and fructose, respectively, which are not considered free sugars. Higher contribution to fiber intakes was provided by fruits, cereals, vegetables and bakery and pastry. There were no significant differences in relation with the total sugar intake according to the body mass index (BMI) between SRS and AMS. The present study suggests a high proportion of children had total carbohydrates intakes in line with recommendations by public health authorities, but still a significant number presented insufficient total carbohydrate and fiber intakes, while total sugar consumption was high, with no major differences between SRS and AMS cohorts.
Keywords: EsNuPI study; Spanish children; carbohydrate intakes; dietary habits; feeding behavior; nutrition assessment; pediatric nutrition; pediatrics; total sugar.
Conflict of interest statement
The funding sponsor had no role in the design of the study, in the collection, analyses or interpretation of the data; in the writing of the manuscript and in the decision to publish the results. The authors declare no conflict of interest, with the exception of Federico Lara, who is a member of the IPN.
Figures
Similar articles
-
Dietary Intake, Nutritional Adequacy, and Food Sources of Protein and Relationships with Personal and Family Factors in Spanish Children Aged One to <10 Years: Findings of the EsNuPI Study.Nutrients. 2021 Mar 24;13(4):1062. doi: 10.3390/nu13041062. Nutrients. 2021. PMID: 33805229 Free PMC article.
-
Dietary Intake of Individual (Intrinsic and Added) Sugars and Food Sources from Spanish Children Aged One to <10 Years—Results from the EsNuPI Study.Nutrients. 2022 Apr 16;14(8):1667. doi: 10.3390/nu14081667. Nutrients. 2022. PMID: 35458229 Free PMC article.
-
Dietary Intake, Nutritional Adequacy and Food Sources of Total Fat and Fatty Acids, and Relationships with Personal and Family Factors in Spanish Children Aged One to <10 Years: Results of the EsNuPI Study.Nutrients. 2020 Aug 16;12(8):2467. doi: 10.3390/nu12082467. Nutrients. 2020. PMID: 32824377 Free PMC article.
-
Sugar in Infants, Children and Adolescents: A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition.J Pediatr Gastroenterol Nutr. 2017 Dec;65(6):681-696. doi: 10.1097/MPG.0000000000001733. J Pediatr Gastroenterol Nutr. 2017. PMID: 28922262 Review.
-
A review of total & added sugar intakes and dietary sources in Europe.Nutr J. 2017 Jan 21;16(1):6. doi: 10.1186/s12937-016-0225-2. Nutr J. 2017. PMID: 28109280 Free PMC article. Review.
Cited by
-
Dietary Intake, Nutritional Adequacy, and Food Sources of Protein and Relationships with Personal and Family Factors in Spanish Children Aged One to <10 Years: Findings of the EsNuPI Study.Nutrients. 2021 Mar 24;13(4):1062. doi: 10.3390/nu13041062. Nutrients. 2021. PMID: 33805229 Free PMC article.
-
Research on commercial milk formulas for young children: A scoping review.Matern Child Nutr. 2024 Oct;20(4):e13675. doi: 10.1111/mcn.13675. Epub 2024 Jul 2. Matern Child Nutr. 2024. PMID: 38956436 Free PMC article.
-
Diet Quality and Nutritional Assessment of Menus Served in Spanish Defense Ministry Preschool Canteens.Nutrients. 2025 Feb 12;17(4):661. doi: 10.3390/nu17040661. Nutrients. 2025. PMID: 40004989 Free PMC article.
-
Cross-Sectional Assessment of Nutritional Status, Dietary Intake, and Physical Activity Levels in Children (6-9 Years) in Valencia (Spain) Using Nutrimetry.Nutrients. 2024 Aug 10;16(16):2649. doi: 10.3390/nu16162649. Nutrients. 2024. PMID: 39203786 Free PMC article.
-
Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders.Nutrients. 2021 Oct 10;13(10):3551. doi: 10.3390/nu13103551. Nutrients. 2021. PMID: 34684552 Free PMC article.
References
-
- Forouzanfar M.H., Afshin A., Alexander L.T., Anderson H.R., Bhutta Z.A., Biryukov S., Brauer M., Burnett R., Cercy K., Charlson F.J., et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1659–1724. doi: 10.1016/S0140-6736(16)31679-8. - DOI - PMC - PubMed
-
- Afshin A., Sur P.J., Fay K.A., Cornaby L., Ferrara G., Salama J.S., Mullany E.C., Abate K.H., Abbafati C., Abebe Z., et al. Health effects of dietary risks in 195 countries, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393:1958–1972. doi: 10.1016/S0140-6736(19)30041-8. - DOI - PMC - PubMed
-
- World Health Organization Global Strategy on Diet, Physical Activity and Health. [(accessed on 18 June 2020)];Childhood Overweight and Obesity. Available online: https://www.who.int/dietphysicalactivity/childhood/en/
-
- Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales. Encuesta Nacional de Salud 2017. Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales; Madrid, Spain: 2018.
