Survival Benefits From Surgery for Stage IVa Head and Neck Squamous Cell Carcinoma: A Multi-institutional Analysis of 1,033 Cases
- PMID: 33081440
- PMCID: PMC8111393
- DOI: 10.21053/ceo.2020.01732
Survival Benefits From Surgery for Stage IVa Head and Neck Squamous Cell Carcinoma: A Multi-institutional Analysis of 1,033 Cases
Abstract
Objectives: Head and neck squamous cell carcinomas (HNSCs) are frequently diagnosed at the locoregional advanced stage (stage IVa), but controversy remains regarding whether stage IVa HSNCs should be treated with upfront surgery or definitive chemoradiation therapy (CRT). The purpose of this study was to compare overall survival (OS) and disease-free survival (DFS) in patients with stage IVa HNSC treated primarily by surgery with curative intent with/without (neo)adjuvant treatment (surgery group) versus those treated primarily with CRT (CRT group).
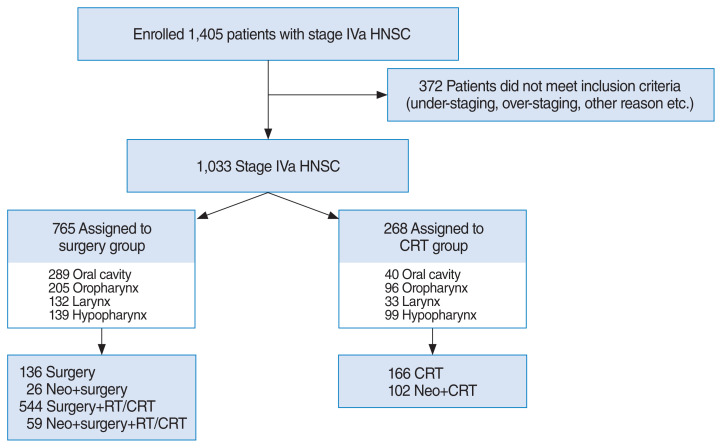
Methods: We reviewed data of 1,033 patients with stage IVa HNSC treated with curative intent at 17 cancer centers between 2010 and 2016.
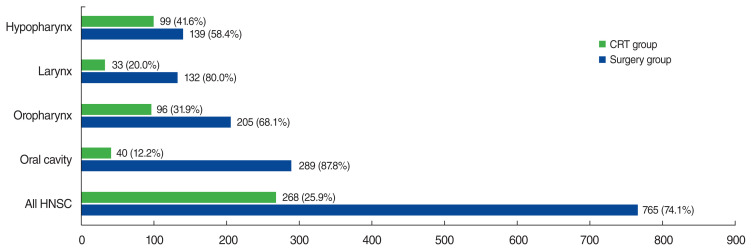
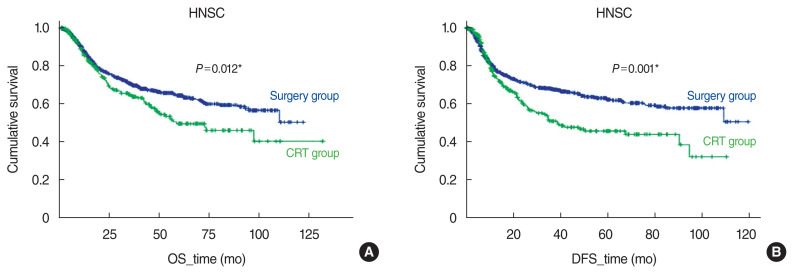
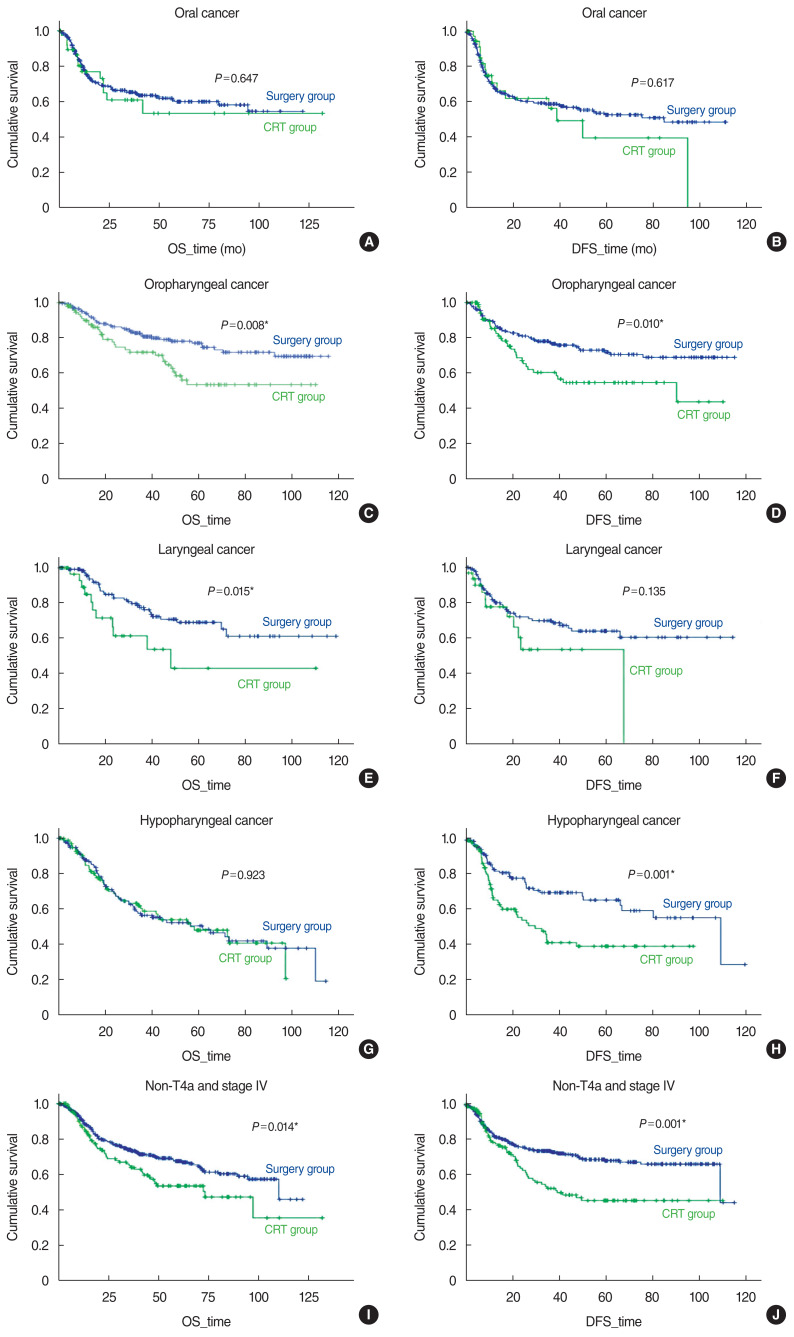
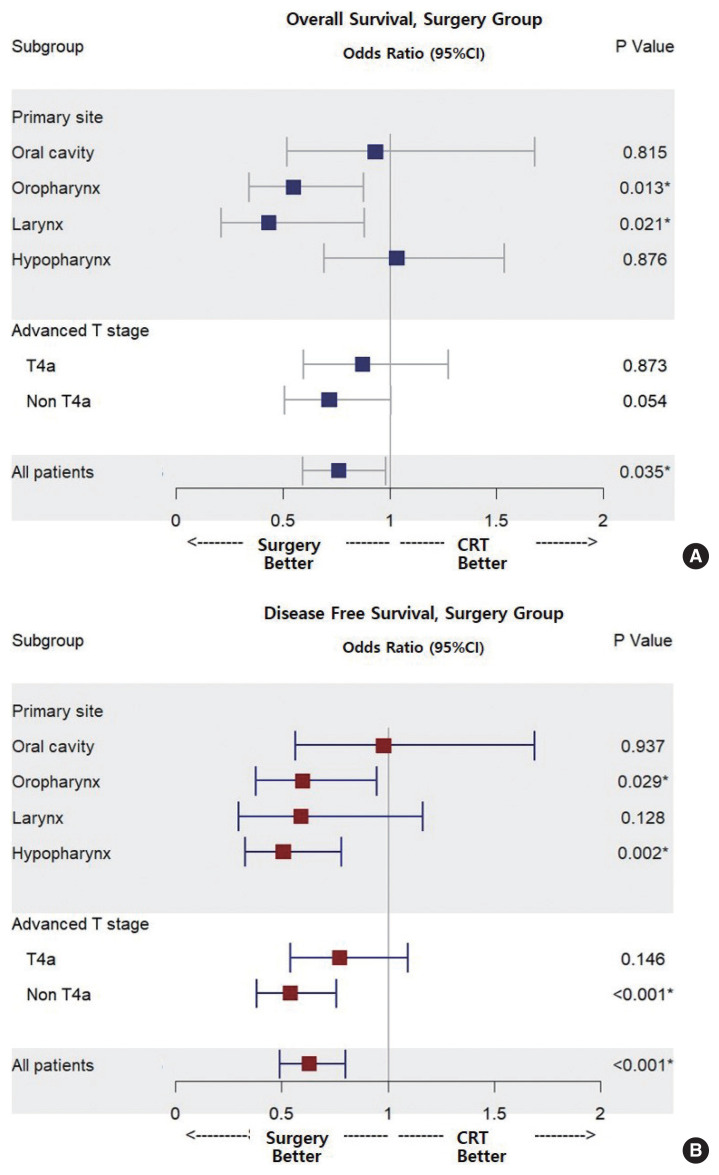
Results: Among 1,033 patients, 765 (74.1%) received upfront surgery and 268 (25.9%) received CRT. The 5-year OS and DFS rates were 64.4% and 62.0% in the surgery group and 49.5% and 45.4% in the CRT group, respectively. In multivariate analyses, OS and DFS were better in the surgery group than in the CRT group (odds ratio [OR] for death, 0.762; 95% confidence interval [CI], 0.592-0.981; OR for recurrence, 0.628; 95% CI, 0.492-0.802). In subgroup analyses, the OS and DFS of patients with oropharyngeal cancer were better in the surgery group (OR for death, 0.548; 95% CI, 0.341-0.879; OR for recurrence, 0.598; 95% CI, 0.377-0.948). In the surgery group, patients with laryngeal cancer showed better OS (OR for death, 0.432; 95% CI, 0.211-0.882), while those with hypopharyngeal cancer DFS was improved (OR for recurrence, 0.506; 95% CI, 0.328-0.780).
Conclusion: A survival benefit from surgery may be achieved even in patients with stage IVa HNSC, particularly those with oropharyngeal and laryngeal cancer. Surgery led to a reduction in the recurrence rate in patients with hypopharyngeal cancer.
Keywords: Hypopharyngeal Neoplasms; Laryngeal Neoplasms; Oral Neoplasms; Oropharyngeal Neoplasm; Prognosis; Squamous Cell Carcinoma of Head And Neck; Surgery; Survival Rate; Survival, Disease-Free Survival.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394–424. - PubMed
-
- Thompson-Harvey A, Yetukuri M, Hansen AR, Simpson MC, Adjei Boakye E, Varvares MA, et al. Rising incidence of late-stage head and neck cancer in the United States. Cancer. 2020 Mar;126(5):1090–101. - PubMed
-
- Gatta G, Botta L, Sanchez MJ, Anderson LA, Pierannunzio D, Licitra L, et al. Prognoses and improvement for head and neck cancers diagnosed in Europe in early 2000s: The EUROCARE-5 population-based study. Eur J Cancer. 2015 Oct;51(15):2130–43. - PubMed
-
- Denis F, Garaud P, Bardet E, Alfonsi M, Sire C, Germain T, et al. Final results of the 94–01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol. 2004 Jan;22(1):69–76. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials