

Machine learning techniques for mortality prediction in critical traumatic patients: anatomic and physiologic variables from the RETRAUCI study
- PMID: 33081694
- PMCID: PMC7576744
- DOI: 10.1186/s12874-020-01151-3
Machine learning techniques for mortality prediction in critical traumatic patients: anatomic and physiologic variables from the RETRAUCI study
Abstract
Background: Interest in models for calculating the risk of death in traumatic patients admitted to ICUs remains high. These models use variables derived from the deviation of physiological parameters and/or the severity of anatomical lesions with respect to the affected body areas. Our objective is to create different predictive models of the mortality of critically traumatic patients using machine learning techniques.
Methods: We used 9625 records from the RETRAUCI database (National Trauma Registry of 52 Spanish ICUs in the period of 2015-2019). Hospital mortality was 12.6%. Data on demographic variables, affected anatomical areas and physiological repercussions were used. The Weka Platform was used, along with a ten-fold cross-validation for the construction of nine supervised algorithms: logistic regression binary (LR), neural network (NN), sequential minimal optimization (SMO), classification rules (JRip), classification trees (CT), Bayesian networks (BN), adaptive boosting (ADABOOST), bootstrap aggregating (BAGGING) and random forest (RFOREST). The performance of the models was evaluated by accuracy, specificity, precision, recall, F-measure, and AUC.
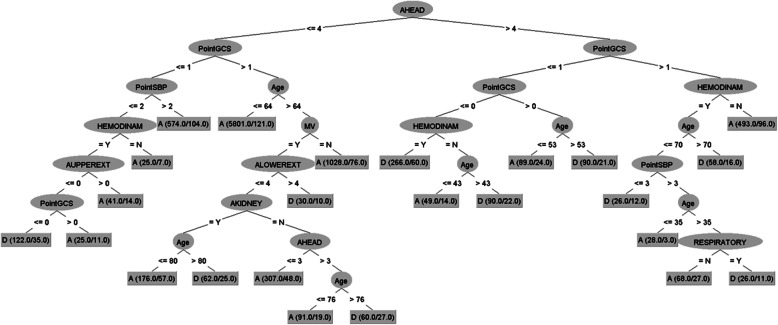
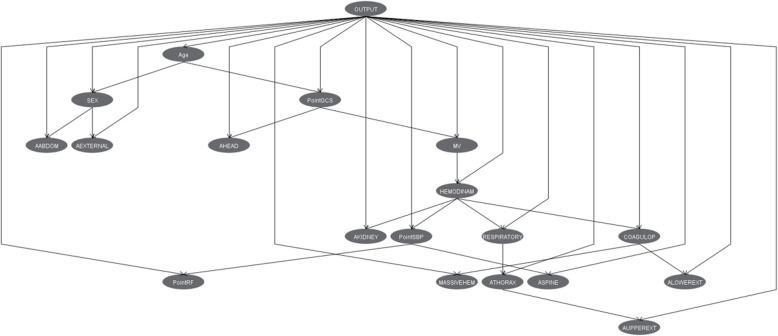
Results: In all algorithms, the most important factors are those associated with traumatic brain injury (TBI) and organic failures. The LR finds thorax and limb injuries as independent protective factors of mortality. The CT generates 24 decision rules and uses those related to TBI as the first variables (range 2.0-81.6%). The JRip detects the eight rules with the highest risk of mortality (65.0-94.1%). The NN model uses a hidden layer of ten nodes, which requires 200 weights for its interpretation. The BN find the relationships between the different factors that identify different patient profiles. Models with the ensemble methodology (ADABOOST, BAGGING and RandomForest) do not have greater performance. All models obtain high values in accuracy, specificity, and AUC, but obtain lower values in recall. The greatest precision is achieved by the SMO model, and the BN obtains the best recall, F-measure, and AUC.
Conclusion: Machine learning techniques are useful for creating mortality classification models in critically traumatic patients. With clinical interpretation, the algorithms establish different patient profiles according to the relationship between the variables used, determine groups of patients with different evolutions, and alert clinicians to the presence of rules that indicate the greatest severity.
Keywords: Intensive care unit; Machine learning techniques; Mortality; Supervised algorithms; Traumatic patient.
Conflict of interest statement
The authors report no conflicts of interests related to the work described.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
