

Relevant factors for early liver transplantation after Kasai portoenterostomy
- PMID: 33081738
- PMCID: PMC7574207
- DOI: 10.1186/s12887-020-02355-8
Relevant factors for early liver transplantation after Kasai portoenterostomy
Abstract
Background: To explore the relevant factors for early liver transplantation (LT) after Kasai portoenterostomy (KP).
Methods: Retrospective analysis was performed for 200 children with biliary atresia, who underwent LT with hepatic failure after KP. According to the interval between KP and LT, they were divided into three groups: G1 (≤6-month), G2 (6-month~ 2-year) and G3 (> 2-year). Gender, age of Kasai portoenterostomy, jaundice-clearance, cholangitis after KP and liver function indexes before LT were compared among the three groups.
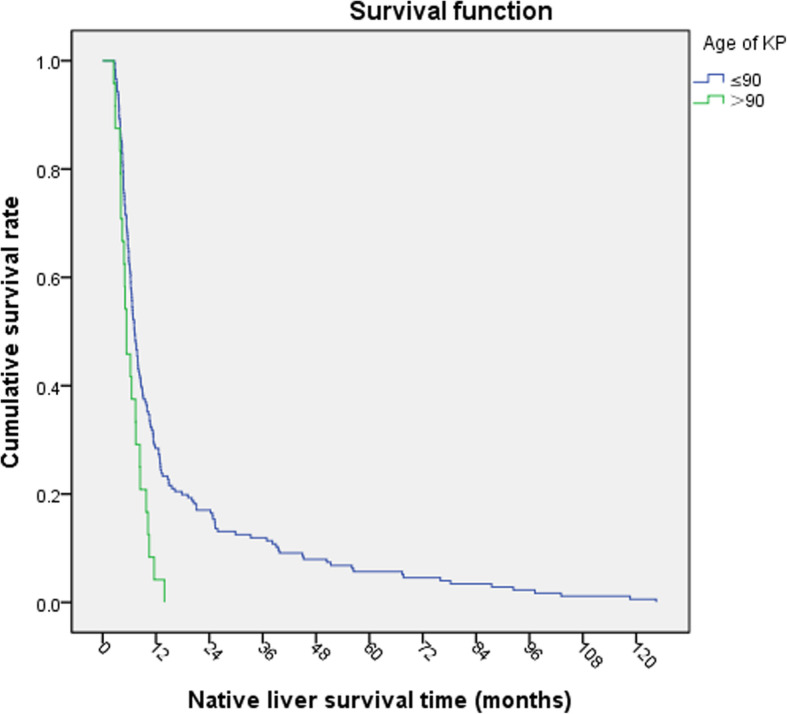
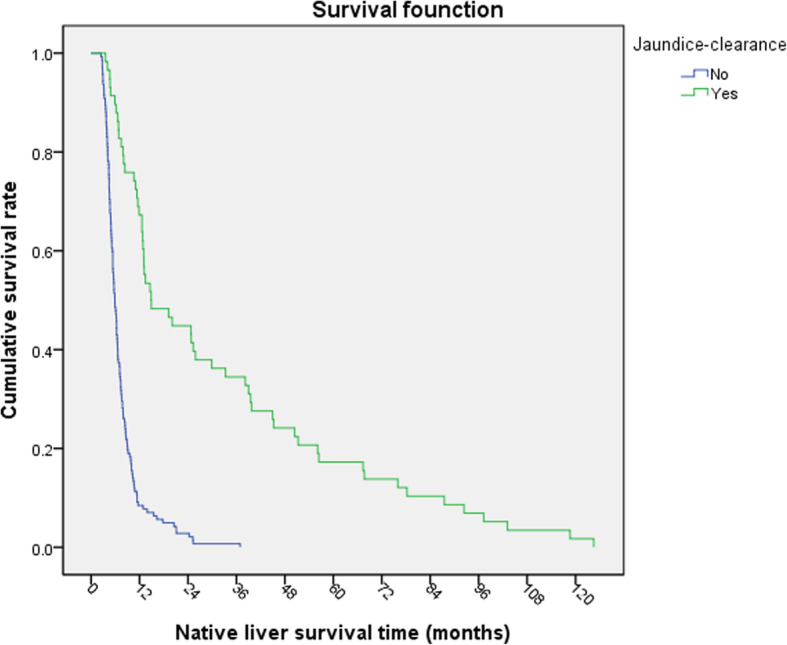
Results: The proportion of patients with age of KP (≤90-day) in G1 was lower than that in G3 (P = 0.003). Jaundice-clearance occurred in 6 (7.6%), 26(28.6%) and 26 (86.7%) patients after KP in G1, G2 and G3 respectively (P < 0.001). There were statistical differences in the incidence of early cholangitis, late cholangitis and repeated cholangitis among the three groups (P = 0.035, < 0.001 and 0.022). The native liver survival (NLS) rate of children at operation age > 90-day was lower than that of children at operation age ≤ 90-day (P = 0.002). The NLS rate of the children with jaundice-clearance after KP was significantly better than that of the children without jaundice-clearance (P < 0.001). The NLS rate of the children with early cholangitis after operation was lower than that in children without early cholangitis (P = 0.026). The NLS rate of patients of G2 and G3 with cholangitis after KP was lower than that in children without cholangitis (P = 0.017). Multiple logistic regression analysis showed uncleared jaundice after KP was a risk factor for the NLS time in patients.
Conclusion: The age of KP (> 90-day), jaundice-unclear and early cholangitis could reduce the NLS time after KP, which were related to early liver transplantation. Jaundice-unclear was a risk factor for early liver transplantation.
Keywords: Biliary atresia; Kasai portoenterostomy; Liver transplantation; Relevant factors.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Five-year native liver survival analysis in biliary atresia from a single large Chinese center: The death/liver transplantation hazard change and the importance of rapid early clearance of jaundice.J Pediatr Surg. 2019 Aug;54(8):1680-1685. doi: 10.1016/j.jpedsurg.2018.09.025. Epub 2018 Oct 30. J Pediatr Surg. 2019. PMID: 30518490
-
Number of cholangitis episodes as a prognostic marker to predict timing of liver transplantation in biliary atresia patients after Kasai portoenterostomy.BMC Pediatr. 2018 Apr 2;18(1):119. doi: 10.1186/s12887-018-1074-2. BMC Pediatr. 2018. PMID: 29606115 Free PMC article.
-
Seventeen years of Kasai portoenterostomy for biliary atresia in a single Southeast Asian paediatric centre.J Paediatr Child Health. 2017 Apr;53(4):412-415. doi: 10.1111/jpc.13379. Epub 2016 Nov 8. J Paediatr Child Health. 2017. PMID: 27859955
-
Revision Kasai portoenterostomy: A review of indications and outcomes.Semin Pediatr Surg. 2024 Dec;33(6):151476. doi: 10.1016/j.sempedsurg.2025.151476. Epub 2025 Jan 16. Semin Pediatr Surg. 2024. PMID: 39881457 Review.
-
Biliary atresia--a fifteen-year review of clinical and pathologic factors associated with liver transplantation.J Pediatr Surg. 2004 Jun;39(6):800-3. doi: 10.1016/j.jpedsurg.2004.02.020. J Pediatr Surg. 2004. PMID: 15185199 Review.
Cited by
-
Major surgical conditions of childhood and their lifelong implications: comprehensive review.BJS Open. 2024 May 8;8(3):zrae028. doi: 10.1093/bjsopen/zrae028. BJS Open. 2024. PMID: 38776252 Free PMC article. Review.
-
A convenient nomogram for predicting early death or liver transplantation after the Kasai procedure in patients with biliary atresia.Langenbecks Arch Surg. 2024 Jan 8;409(1):30. doi: 10.1007/s00423-023-03216-5. Langenbecks Arch Surg. 2024. PMID: 38189999
-
A Novel Model for Predicting the Clearance of Jaundice in Patients With Biliary Atresia After Kasai Procedure.Front Pediatr. 2022 Jan 31;10:837247. doi: 10.3389/fped.2022.837247. eCollection 2022. Front Pediatr. 2022. PMID: 35174110 Free PMC article.
-
The favorable prognosis of cystic biliary atresia may be related to early surgery and mild liver pathological changes.Pediatr Surg Int. 2022 Feb;38(2):217-224. doi: 10.1007/s00383-021-05030-w. Epub 2021 Oct 7. Pediatr Surg Int. 2022. PMID: 34618182
-
Treatment of intractable cholangitis in children with biliary atresia: Impact on outcome.Indian J Gastroenterol. 2023 Apr;42(2):209-218. doi: 10.1007/s12664-022-01328-2. Epub 2023 Apr 14. Indian J Gastroenterol. 2023. PMID: 37058274
References
-
- Zhong ZH, Chen HD, Huang LE, et al. 20-year transplant-free survival of biliary atresia after Kasai operation. Chin J Pediatr Surg. 2014;35(4):265–268. doi: 10.3760/cma.j.issn.0253-3006.2014.04.007. - DOI
-
- Zhu ZJ, Sun LY, Wei L, et al. Liver transplantation for the treatment of biliary atresia in children: a report of 130 cases. Chin J Pediatr Surg. 2014;35(4):259–264. doi: 10.3760/cma.j.issn.0253-3006.2014.04.006. - DOI
-
- Zhan JH, Feng JX. When should the biliary atresia perform Kasai procedure. Chin J Pediatr Surg. 2016;37(5):321–326.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
