

Global estimation of anti-malarial drug effectiveness for the treatment of uncomplicated Plasmodium falciparum malaria 1991-2019
- PMID: 33081784
- PMCID: PMC7573874
- DOI: 10.1186/s12936-020-03446-8
Global estimation of anti-malarial drug effectiveness for the treatment of uncomplicated Plasmodium falciparum malaria 1991-2019
Abstract
Background: Anti-malarial drugs play a critical role in reducing malaria morbidity and mortality, but their role is mediated by their effectiveness. Effectiveness is defined as the probability that an anti-malarial drug will successfully treat an individual infected with malaria parasites under routine health care delivery system. Anti-malarial drug effectiveness (AmE) is influenced by drug resistance, drug quality, health system quality, and patient adherence to drug use; its influence on malaria burden varies through space and time.
Methods: This study uses data from 232 efficacy trials comprised of 86,776 infected individuals to estimate the artemisinin-based and non-artemisinin-based AmE for treating falciparum malaria between 1991 and 2019. Bayesian spatiotemporal models were fitted and used to predict effectiveness at the pixel-level (5 km × 5 km). The median and interquartile ranges (IQR) of AmE are presented for all malaria-endemic countries.
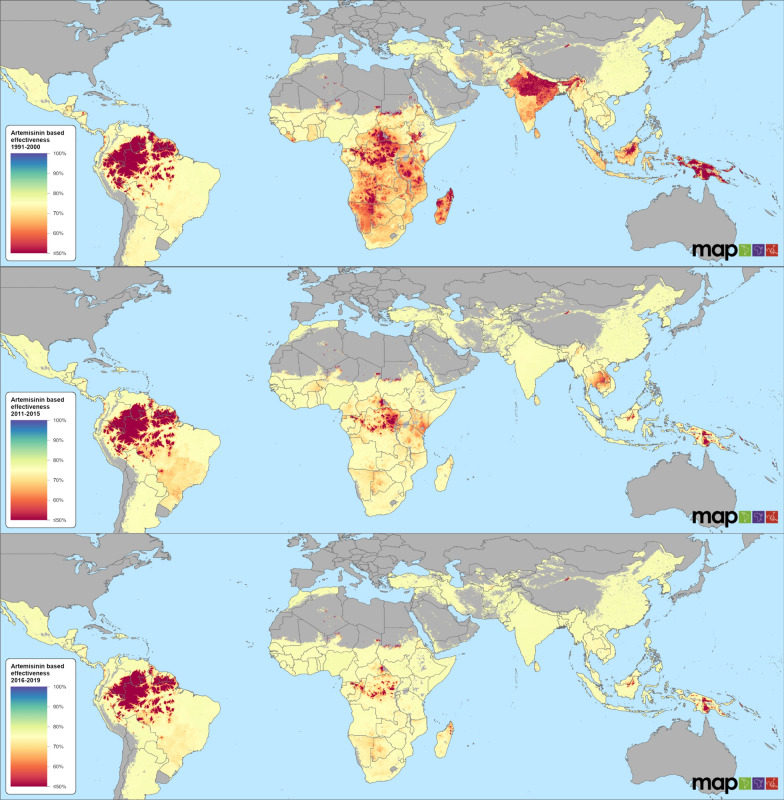
Results: The global effectiveness of artemisinin-based drugs was 67.4% (IQR: 33.3-75.8), 70.1% (43.6-76.0) and 71.8% (46.9-76.4) for the 1991-2000, 2006-2010, and 2016-2019 periods, respectively. Countries in central Africa, a few in South America, and in the Asian region faced the challenge of lower effectiveness of artemisinin-based anti-malarials. However, improvements were seen after 2016, leaving only a few hotspots in Southeast Asia where resistance to artemisinin and partner drugs is currently problematic and in the central Africa where socio-demographic challenges limit effectiveness. The use of artemisinin-based combination therapy (ACT) with a competent partner drug and having multiple ACT as first-line treatment choice sustained high levels of effectiveness. High levels of access to healthcare, human resource capacity, education, and proximity to cities were associated with increased effectiveness. Effectiveness of non-artemisinin-based drugs was much lower than that of artemisinin-based with no improvement over time: 52.3% (17.9-74.9) for 1991-2000 and 55.5% (27.1-73.4) for 2011-2015. Overall, AmE for artemisinin-based and non-artemisinin-based drugs were, respectively, 29.6 and 36% below clinical efficacy as measured in anti-malarial drug trials.
Conclusions: This study provides evidence that health system performance, drug quality and patient adherence influence the effectiveness of anti-malarials used in treating uncomplicated falciparum malaria. These results provide guidance to countries' treatment practises and are critical inputs for malaria prevalence and incidence models used to estimate national level malaria burden.
Keywords: Anti-malarial drug effectiveness; Drug quality; Falciparum malaria; Global.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- GBD 2017 Mortality Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- WHO . World malaria report 2014. Geneva: World Health Organization; 2014.
-
- WHO . Key points: World malaria report. Geneva: World Health Organization; 2017.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
