

Automated computed tomography quantification of fibrosis predicts prognosis in combined pulmonary fibrosis and emphysema in a real-world setting: a single-centre, retrospective study
- PMID: 33081788
- PMCID: PMC7576807
- DOI: 10.1186/s12931-020-01545-3
Automated computed tomography quantification of fibrosis predicts prognosis in combined pulmonary fibrosis and emphysema in a real-world setting: a single-centre, retrospective study
Abstract
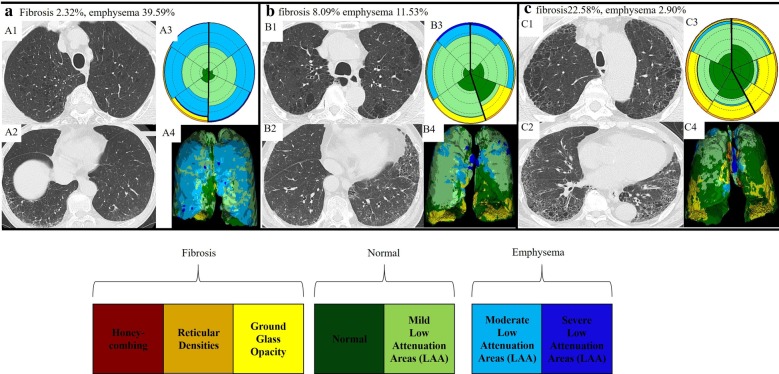
Background: Combined pulmonary fibrosis and emphysema (CPFE) is a heterogeneous clinico-radiological syndrome without a consensus definition. There are limited data on the relation between the amount of parenchymal fibrosis and prognosis. In this study, we assessed the prognostic implications of the extent of fibrosis assessed by an automated quantitative computed tomography (CT) technique and the radiological and functional change over time in patients with a broad spectrum of fibrotic interstitial lung diseases (ILDs) encountered in a real-world setting.
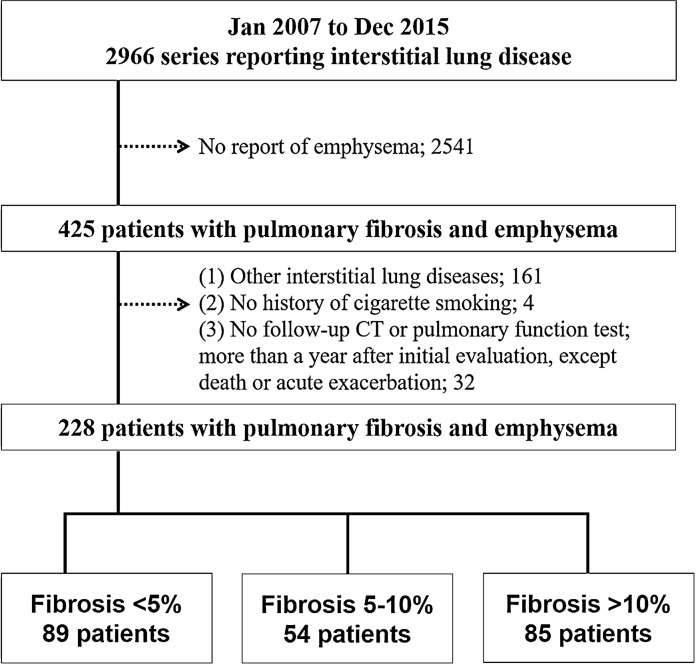
Methods: We conducted a single-centre, retrospective study of 228 consecutive patients with CPFE, encountered from 2007 to 2015 at Kameda Medical Center, Chiba, Japan. We investigated the prognostic value of automated CT fibrosis quantification and the subsequent course of CPFE.
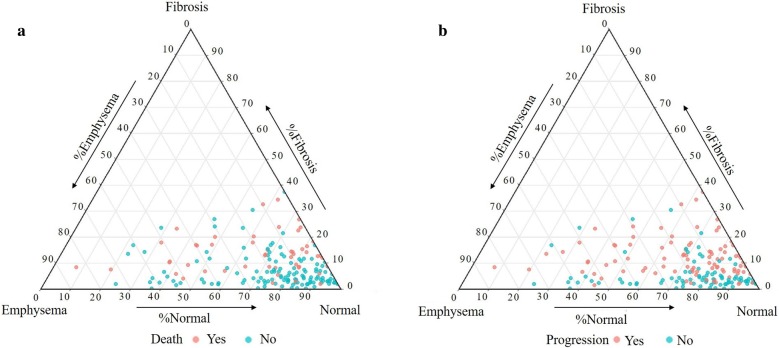
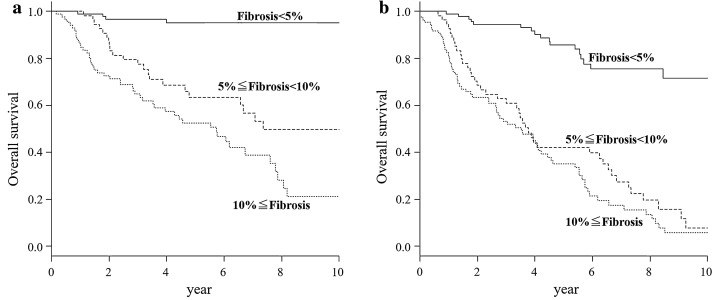
Results: Among 228 patients with CPFE, 89 had fibrosis affecting < 5% of their lungs, 54 had 5 to < 10% fibrosis, and 85 had ≥ 10% fibrosis at the time of diagnosis. Lower volume of fibrosis correlated with lower rates of mortality and acute exacerbation (p < 0.001). In particular, among those with < 5% fibrosis, only 4.5% died and none experienced acute exacerbation during follow-up, whereas 57.6% and 29.4% of those with ≥ 10% fibrosis experienced death and acute exacerbation, respectively. Although, the ≥ 10% fibrosis group had the poorest overall survival as well as the highest incidence of acute exacerbation, the incidence of decline in pulmonary function tests, change per year in total lung volume, and progression of fibrosis on chest CT was highest in the 5 to < 10% fibrosis group. The Cox proportional hazard model for CPFE progression (defined by composite criteria of death, acute exacerbation, and decline in forced vital capacity or diffusing capacity) showed fibrosis proportion was a risk factor independent of age, sex, smoking pack-years, the Charlson Comorbidity Index, lung cancer, connective tissue disease, and idiopathic pulmonary fibrosis.
Conclusions: Less severe (< 5%) fibrosis at baseline was associated with disease stability and better prognosis compared to more severe fibrosis in CPFE occurring with fibrotic ILDs. Further studies including a validation cohort will be needed. Trial Registration Retrospectively registered.
Keywords: Cohort studies; Fibrosis; Lung; Pulmonary emphysema; Tomography.
Conflict of interest statement
Dr. Bartholmai reports royalties from Imbio, LLC, during the conduct of the study. The CALIPER software is licensed to Imbio, LLC and sold as Imbio Lung Texture Analysis (LTA). Royalties are due to Mayo Clinic and Dr. Bartholmai and were paid during this study, but no fees were given to the authors or to Mayo Clinic directly related to the content of the manuscript. Dr. Bartholmai also received personal fees from Promedior, LLC, grants from NIH/NHLBI, personal fees from Imbio, LLC, and Mayo Clinic received fees from Boehringer Ingelheim, outside the submitted work in the last 3 years. In addition, Dr. Bartholmai has a patent systems and methods for analyzing in vivo tissue volumes using medical imaging pending.
Figures
Similar articles
-
Combined pulmonary fibrosis and emphysema and idiopathic pulmonary fibrosis in non-small cell lung cancer: impact on survival and acute exacerbation.BMC Pulm Med. 2019 Oct 15;19(1):177. doi: 10.1186/s12890-019-0951-2. BMC Pulm Med. 2019. PMID: 31615505 Free PMC article.
-
Prognosis of patients with acute exacerbation of combined pulmonary fibrosis and emphysema: a retrospective single-centre study.BMC Pulm Med. 2020 May 20;20(1):144. doi: 10.1186/s12890-020-01185-9. BMC Pulm Med. 2020. PMID: 32434532 Free PMC article.
-
The value of CT for disease detection and prognosis determination in combined pulmonary fibrosis and emphysema (CPFE).PLoS One. 2014 Sep 9;9(9):e107476. doi: 10.1371/journal.pone.0107476. eCollection 2014. PLoS One. 2014. PMID: 25203455 Free PMC article.
-
The impact of emphysema in pulmonary fibrosis.Eur Respir Rev. 2013 Jun 1;22(128):153-7. doi: 10.1183/09059180.00000813. Eur Respir Rev. 2013. PMID: 23728869 Free PMC article. Review.
-
Combined pulmonary fibrosis and emphysema: The many aspects of a cohabitation contract.Respir Med. 2016 Aug;117:14-26. doi: 10.1016/j.rmed.2016.05.005. Epub 2016 May 7. Respir Med. 2016. PMID: 27492509 Review.
Cited by
-
ILD-GAP Combined with the Charlson Comorbidity Index Score (ILD-GAPC) as a Prognostic Prediction Model in Patients with Interstitial Lung Disease.Can Respir J. 2023 Feb 8;2023:5088207. doi: 10.1155/2023/5088207. eCollection 2023. Can Respir J. 2023. PMID: 36817552 Free PMC article.
-
Chronic Obstructive Pulmonary Disease Combined with Interstitial Lung Disease.Tuberc Respir Dis (Seoul). 2022 Apr;85(2):122-136. doi: 10.4046/trd.2021.0141. Epub 2022 Jan 27. Tuberc Respir Dis (Seoul). 2022. PMID: 35385639 Free PMC article. Review.
-
Effect of combined pulmonary fibrosis and emphysema on patients with connective tissue diseases and systemic sclerosis: a systematic review and meta-analysis.Arthritis Res Ther. 2021 Apr 6;23(1):100. doi: 10.1186/s13075-021-02494-y. Arthritis Res Ther. 2021. PMID: 33823923 Free PMC article.
-
Syndrome of Combined Pulmonary Fibrosis and Emphysema: An Official ATS/ERS/JRS/ALAT Research Statement.Am J Respir Crit Care Med. 2022 Aug 15;206(4):e7-e41. doi: 10.1164/rccm.202206-1041ST. Am J Respir Crit Care Med. 2022. PMID: 35969190 Free PMC article.
-
Ectopic and visceral fat deposition in aging, obesity, and idiopathic pulmonary fibrosis: an interconnected role.Lipids Health Dis. 2023 Nov 24;22(1):201. doi: 10.1186/s12944-023-01964-3. Lipids Health Dis. 2023. PMID: 38001499 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
