

Prognostic impact of admission high-sensitivity C-reactive protein in acute myocardial infarction patients with and without diabetes mellitus
- PMID: 33081810
- PMCID: PMC7576820
- DOI: 10.1186/s12933-020-01157-7
Prognostic impact of admission high-sensitivity C-reactive protein in acute myocardial infarction patients with and without diabetes mellitus
Abstract
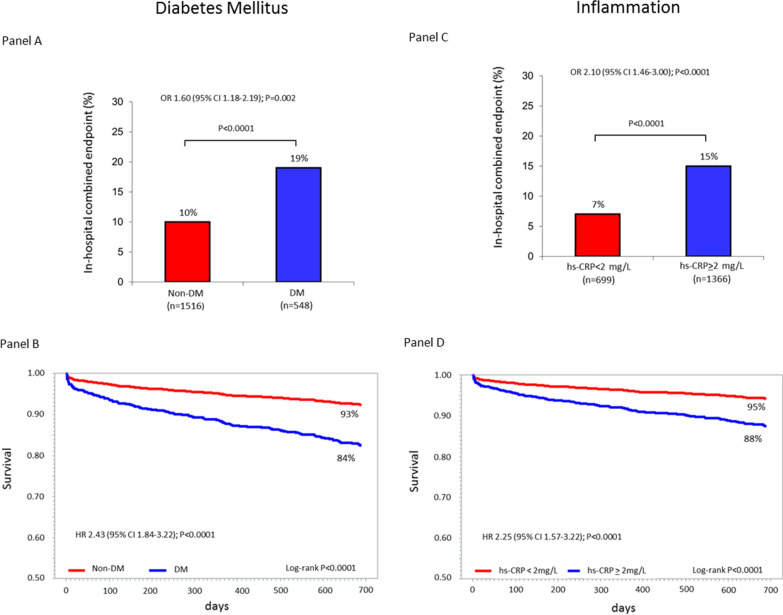
Background: High-sensitivity C-reactive protein (hs-CRP) elevation frequently occurs in acute myocardial infarction (AMI) and is associated with adverse outcomes. Since diabetes mellitus (DM) is characterized by an underlying chronic inflammation, hs-CRP may have a different prognostic power in AMI patients with and without DM.
Methods: We prospectively included 2064 AMI patients; hs-CRP was measured at hospital admission. Patients were grouped according to hs-CRP quartiles and DM status. The primary endpoint was a composite of in-hospital mortality, cardiogenic shock, and acute pulmonary edema. Two-year all-cause mortality was the secondary endpoint.
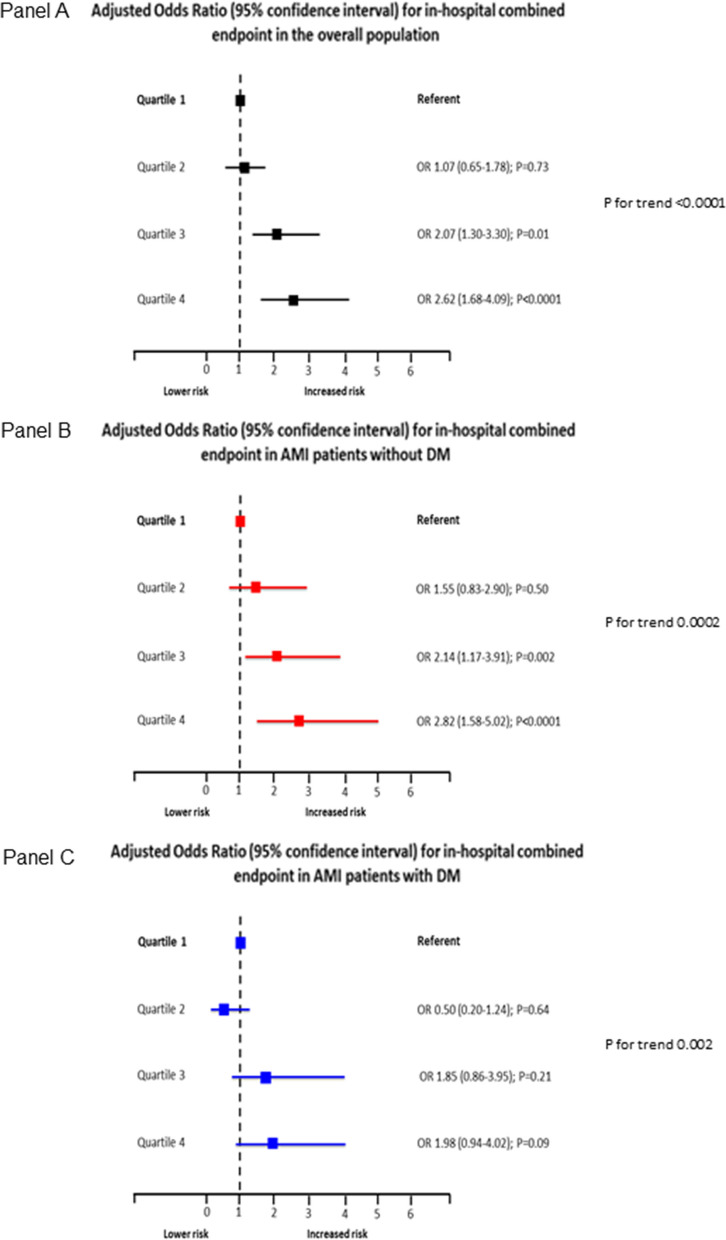
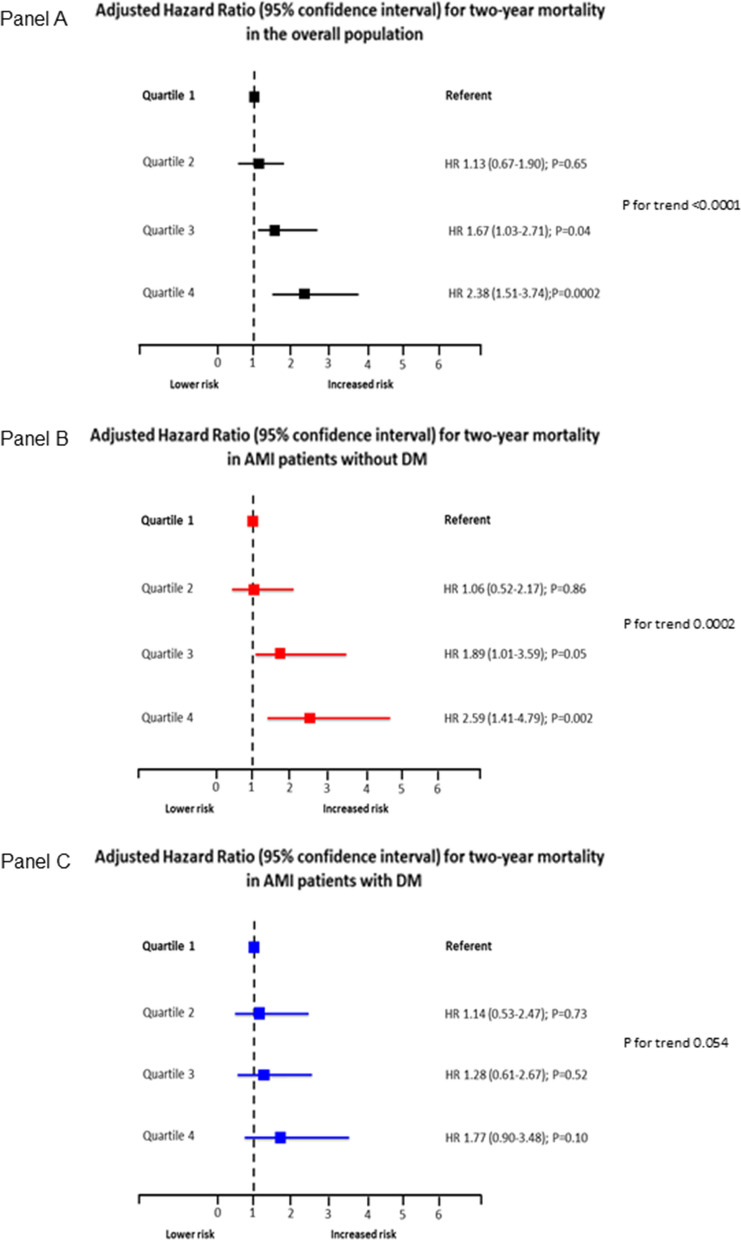
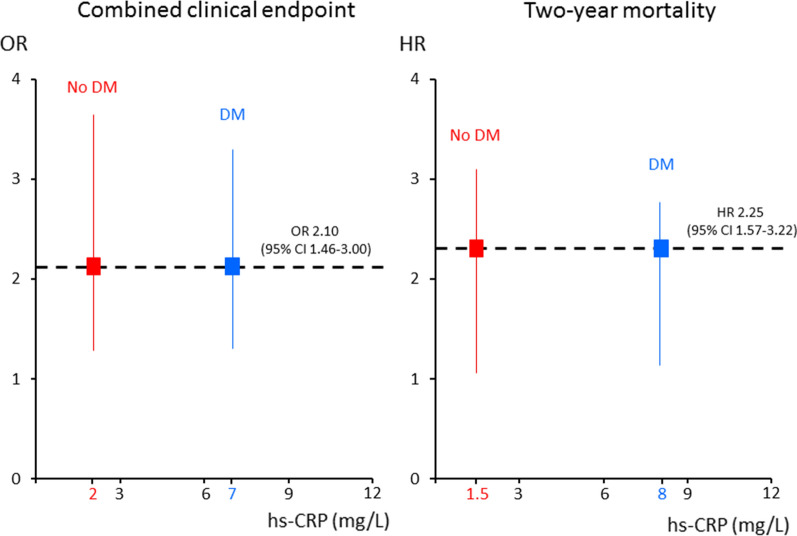
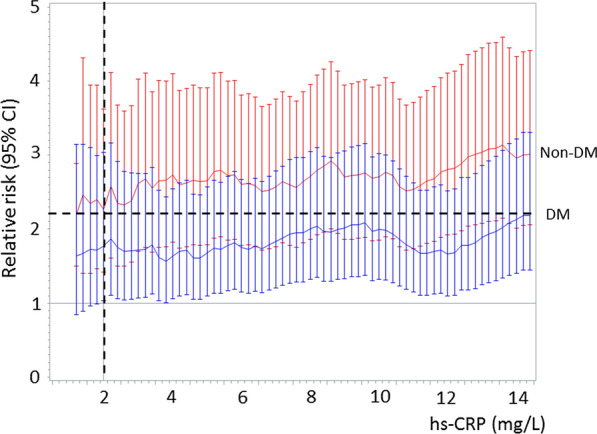
Results: Twenty-six percent (n = 548) of patients had DM and they had higher hs-CRP levels than non-DM patients (5.32 vs. 3.24 mg/L; P < 0.0001). The primary endpoint incidence in the overall population (7%, 9%, 13%, 22%; P for trend < 0.0001), in DM (14%, 9%, 21%, 27%; P = 0.0001), and non-DM (5%, 8%, 10%, 19%; P < 0.0001) patients increased in parallel with hs-CRP quartiles. The adjusted risk of the primary endpoint increased in parallel with hs-CRP quartiles in DM and non-DM patients but this relationship was less evident in DM patients. In the overall population, the adjusted OR of the primary endpoint associated with an hs-CRP value ≥ 2 mg/L was 2.10 (95% CI 1.46-3.00). For the same risk, hs-CRP was 7 and 2 mg/L in patients with and without DM. A similar behavior was observed for the secondary endpoint when the HR associated with an hs-CRP value ≥ 2 mg/L found in the overall population was 2.25 (95% CI 1.57-3.22). For the same risk, hs-CRP was 8 and 1.5 mg/L in DM and non-DM patients.
Conclusions: This study shows that hs-CRP predicts in-hospital outcome and two-year mortality in AMI patients with and without DM. However, in DM patients, the same risk of developing events as in non-DM patients is associated to higher hs-CRP levels.
Keywords: Acute myocardial infarction; Diabetes mellitus; High-sensitivity C-reactive protein; Inflammation.
Conflict of interest statement
none.
Figures
References
-
- Brener SJ, Mehran R, Dressler O, Cristea E, Stone GW. Diabetes mellitus, myocardial reperfusion, and outcome in patients with acute ST-elevation myocardial infarction treated with primary angioplasty (from HORIZONS AMI) Am J Cardiol. 2012;109:1111–1116. doi: 10.1016/j.amjcard.2011.11.046. - DOI - PubMed
-
- Malmberg K, Yusuf S, Gerstein HC, Brown J, Zhao F, Hunt D, Piegas L, Calvin J, Keltai M, Budaj A. Impact of diabetes on long-term prognosis in patients with unstable angina and non-Q-wave myocardial infarction: results of the OASIS (Organization to Assess Strategies for Ischemic Syndromes) Registry. Circulation. 2000;102:1014–1019. doi: 10.1161/01.CIR.102.9.1014. - DOI - PubMed
-
- Marenzi G, Cosentino N, Genovese S, Campodonico J, De Metrio M, Rondinelli M, Cornara S, Somaschini A, Camporotondo R, Demarchi A, Milazzo V, Moltrasio M, Rubino M, Marana I, Grazi M, Lauri G, Bonomi A, Veglia F, De Ferrari GM, Bartorelli AL. Reduced cardio-renal function accounts for most of the in-hospital morbidity and mortality risk among patients with type 2 diabetes undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Diab Care. 2019;42:1305–1311. doi: 10.2337/dc19-0047. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
