

Posterior column osteotomy plus unilateral cage strutting for correction of lumbosacral fractional curve in degenerative lumbar scoliosis
- PMID: 33081812
- PMCID: PMC7574557
- DOI: 10.1186/s13018-020-02011-y
Posterior column osteotomy plus unilateral cage strutting for correction of lumbosacral fractional curve in degenerative lumbar scoliosis
Abstract
Background: Inadequate release of the posterior spinal bone elements may hinder the correction of the lumbosacral fractional curve in degenerative lumbar scoliosis, since the lumbosacral junction tends to be particularly rigid and may already be fused into an abnormal position. The purpose of this study was to evaluate the surgical outcome and complications of posterior column osteotomy plus unilateral cage strutting technique on lumbosacral concavity for correction of fractional curve in degenerative lumbar scoliosis patients.
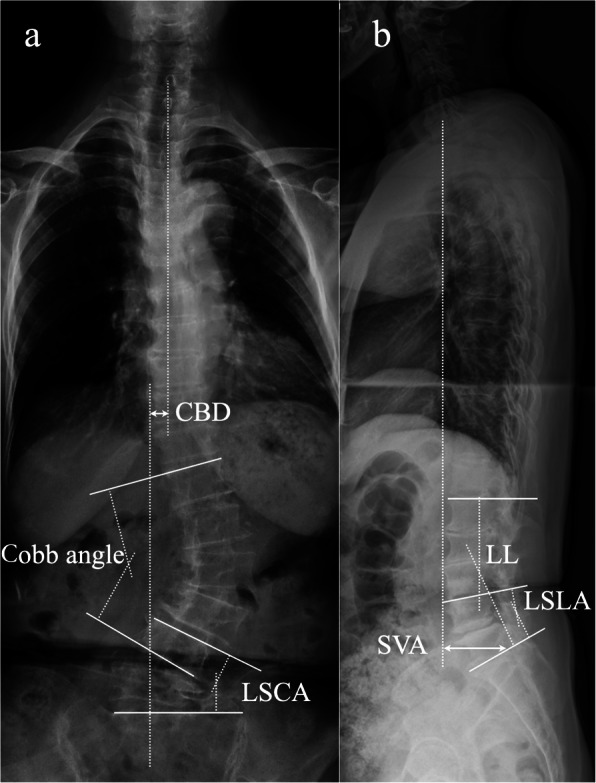
Methods: Thirty-two degenerative lumbar scoliosis patients with lumbosacral fractional curve more than 15° that were surgically treated by posterior column osteotomy plus unilateral cage strutting technique were retrospectively reviewed. The patients' medical records were reviewed to identify demographic and surgical data, including age, sex, body mass index, back pain, leg pain, Oswestry Disability Index, operation time, blood loss, and instrumentation levels. Radiological data including coronal balance distance, Cobb angle, lumbosacral coronal angle, sagittal vertical axis, lumbar lordosis, and lumbosacral lordotic angle were evaluated before and after surgery. Cage subsidence and bone fusion were evaluated at 2-year follow-up.
Results: All patients underwent the operation successfully; lumbosacral coronal angle changed from preoperative 20.1 ± 5.3° to postoperative 5.8 ± 5.7°, with mean correction of 14.3 ± 4.4°, and the correction was maintained at 2-year follow-up. Cobb's angle and coronal balance distance decreased from preoperative to postoperative; the correction was maintained at 2-year follow-up. Sagittal vertical axis decreased, and lumbar lordosis increased from preoperative to postoperative; the correction was also maintained at 2-year follow-up. Lumbosacral lordotic angle presented no change from preoperative to postoperative and from postoperative to 2-year follow-up. Postoperatively, there were 8 patients with lumbosacral coronal angle more than 10°, they got the similar lumbosacral coronal angle correction, but presented larger preoperative Cobb and lumbosacral coronal angle than the other 24 patients. No cage subsidence was detected; all patients achieved intervertebral bone fusion and inter-transverse bone graft fusion at the lumbosacral region at 2-year follow-up.
Conclusion: Posterior column osteotomy plus unilateral cage strutting technique on the lumbosacral concavity facilitate effective correction of the fractional curve in degenerative lumbar scoliosis patients through complete release of dural sac as well as the asymmetrical intervertebral reconstruction by cage.
Keywords: Degenerative lumbar scoliosis; Lumbosacral fractional curve; Posterior column osteotomy; Unilateral cage strutting.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
