

Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: national derivation and validation cohort study
- PMID: 33082154
- PMCID: PMC7574532
- DOI: 10.1136/bmj.m3731
Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: national derivation and validation cohort study
Abstract
Objective: To derive and validate a risk prediction algorithm to estimate hospital admission and mortality outcomes from coronavirus disease 2019 (covid-19) in adults.
Design: Population based cohort study.
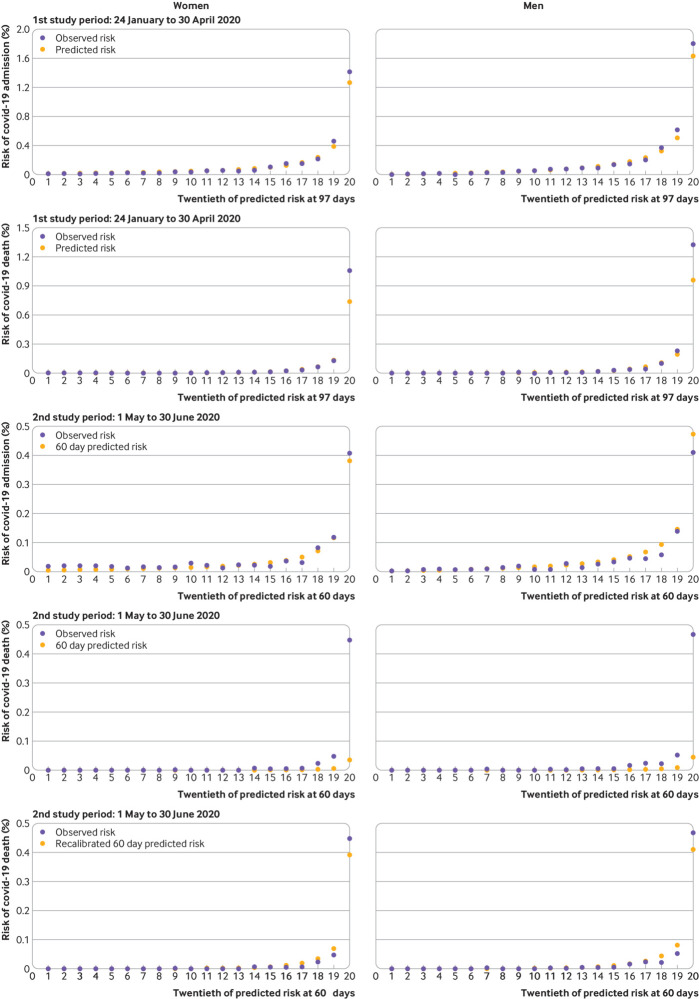
Setting and participants: QResearch database, comprising 1205 general practices in England with linkage to covid-19 test results, Hospital Episode Statistics, and death registry data. 6.08 million adults aged 19-100 years were included in the derivation dataset and 2.17 million in the validation dataset. The derivation and first validation cohort period was 24 January 2020 to 30 April 2020. The second temporal validation cohort covered the period 1 May 2020 to 30 June 2020.
Main outcome measures: The primary outcome was time to death from covid-19, defined as death due to confirmed or suspected covid-19 as per the death certification or death occurring in a person with confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in the period 24 January to 30 April 2020. The secondary outcome was time to hospital admission with confirmed SARS-CoV-2 infection. Models were fitted in the derivation cohort to derive risk equations using a range of predictor variables. Performance, including measures of discrimination and calibration, was evaluated in each validation time period.
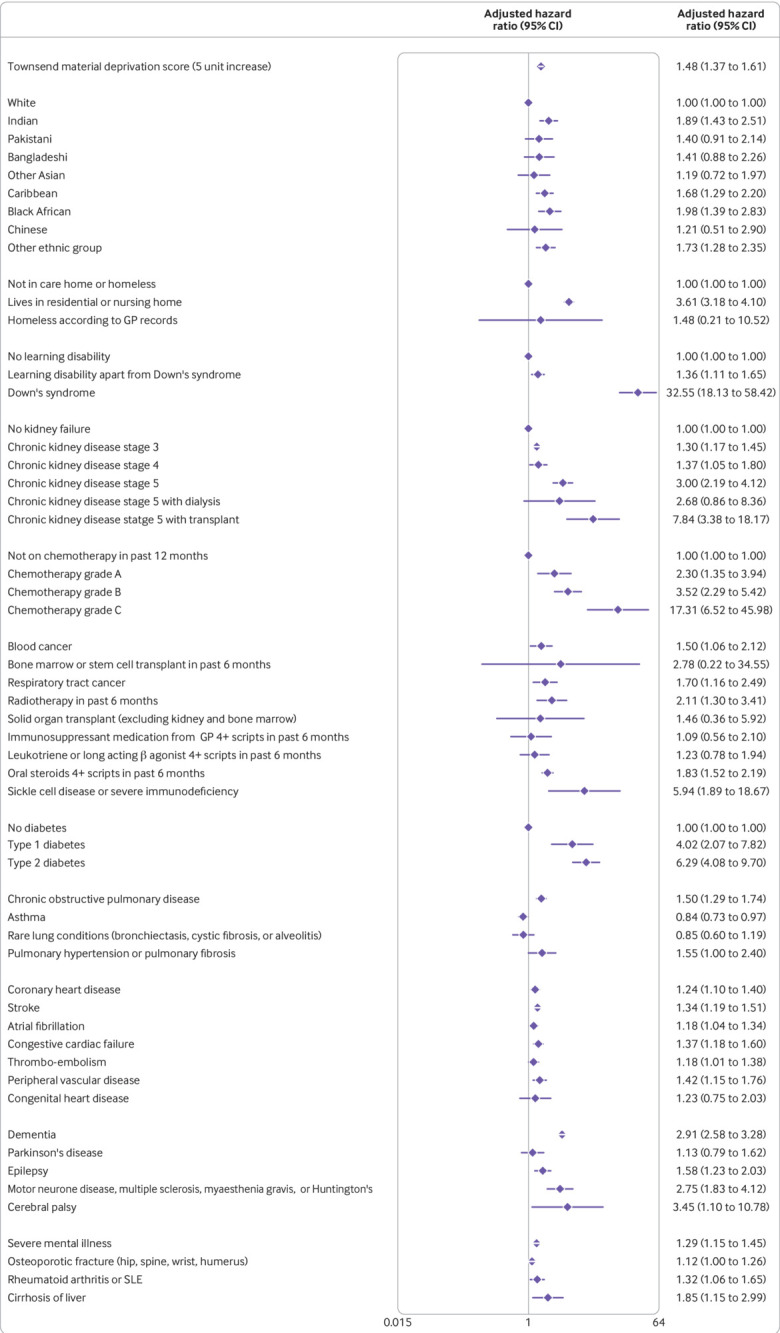
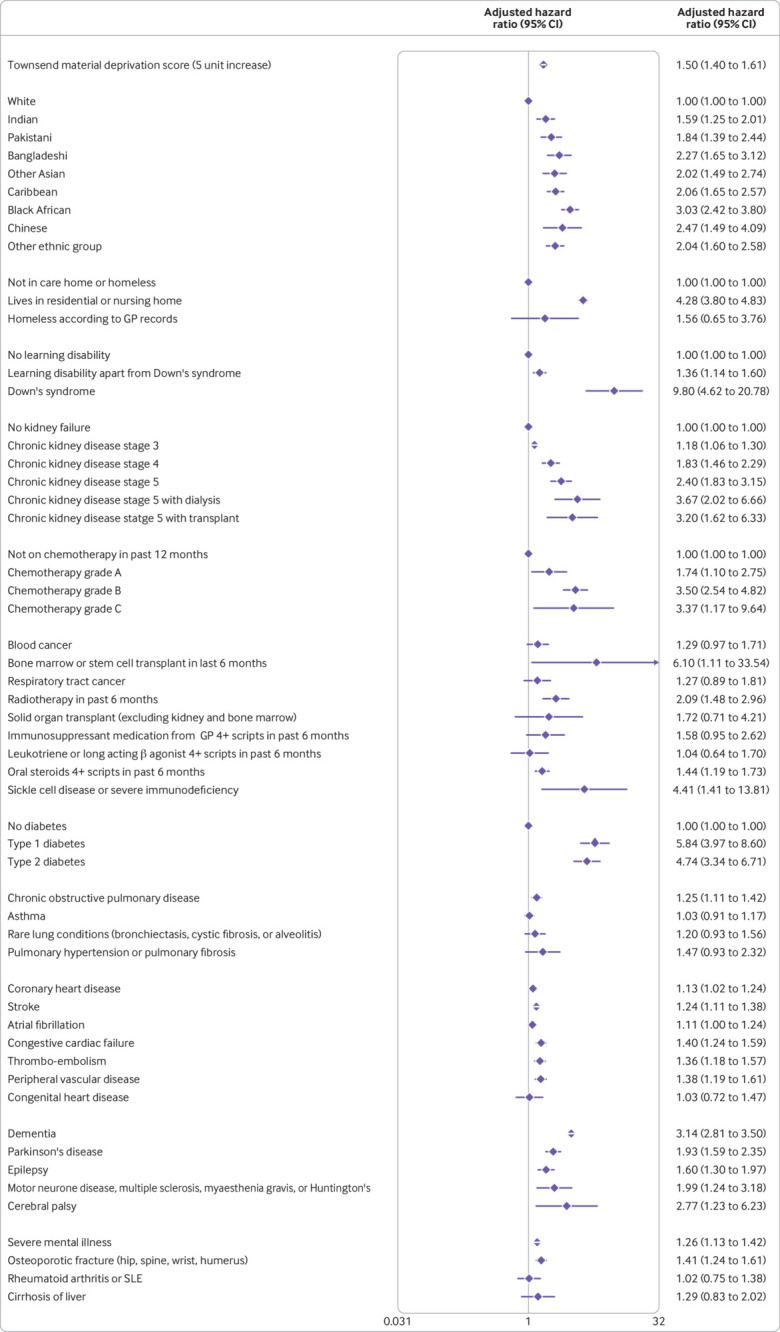
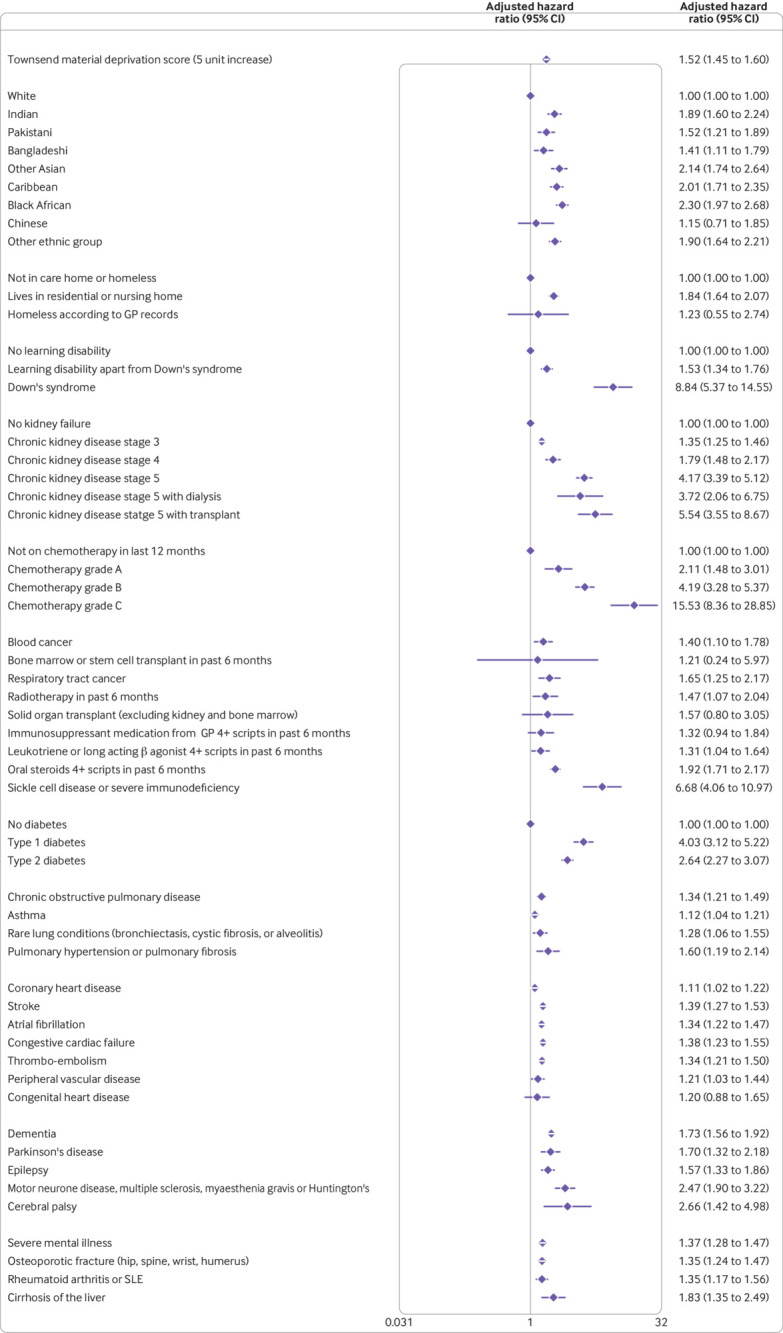
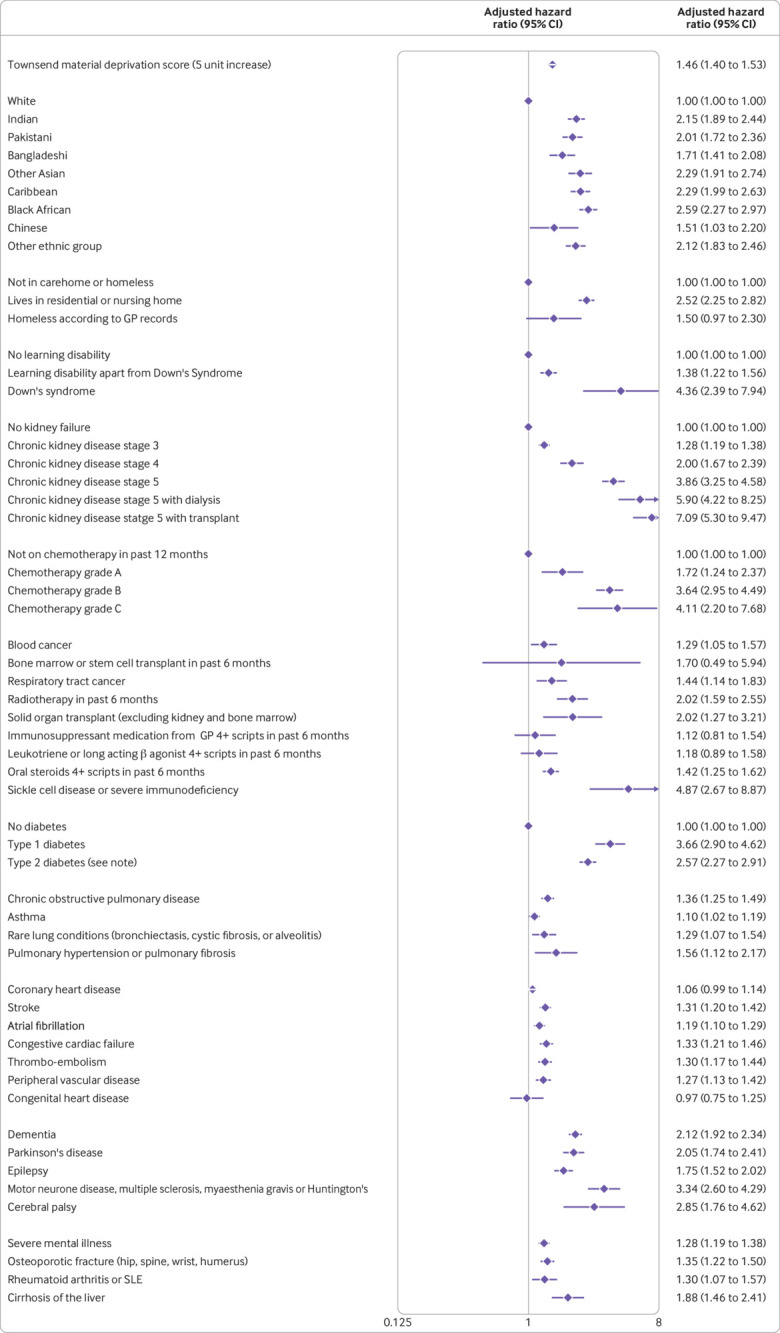
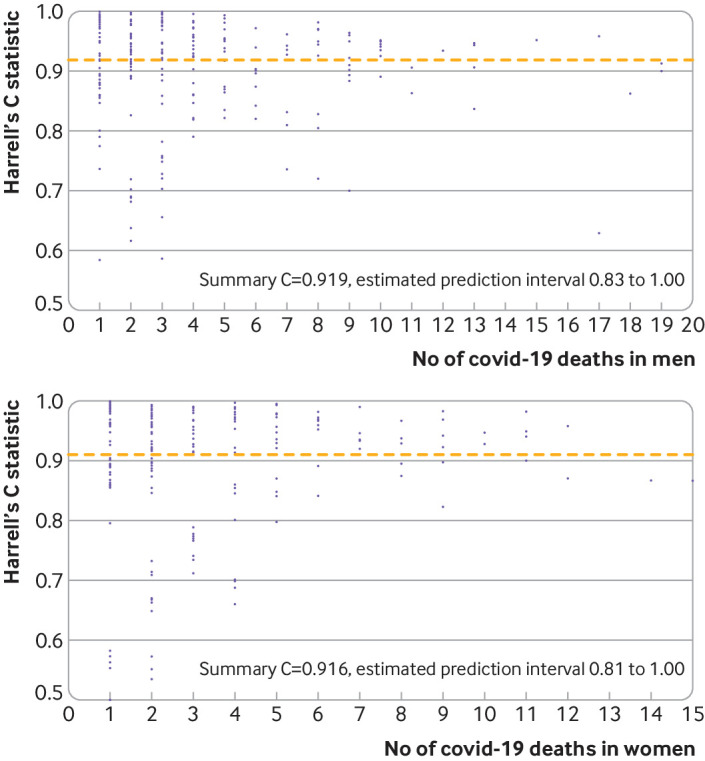
Results: 4384 deaths from covid-19 occurred in the derivation cohort during follow-up and 1722 in the first validation cohort period and 621 in the second validation cohort period. The final risk algorithms included age, ethnicity, deprivation, body mass index, and a range of comorbidities. The algorithm had good calibration in the first validation cohort. For deaths from covid-19 in men, it explained 73.1% (95% confidence interval 71.9% to 74.3%) of the variation in time to death (R2); the D statistic was 3.37 (95% confidence interval 3.27 to 3.47), and Harrell's C was 0.928 (0.919 to 0.938). Similar results were obtained for women, for both outcomes, and in both time periods. In the top 5% of patients with the highest predicted risks of death, the sensitivity for identifying deaths within 97 days was 75.7%. People in the top 20% of predicted risk of death accounted for 94% of all deaths from covid-19.
Conclusion: The QCOVID population based risk algorithm performed well, showing very high levels of discrimination for deaths and hospital admissions due to covid-19. The absolute risks presented, however, will change over time in line with the prevailing SARS-C0V-2 infection rate and the extent of social distancing measures in place, so they should be interpreted with caution. The model can be recalibrated for different time periods, however, and has the potential to be dynamically updated as the pandemic evolves.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: JHC has received grants from the National Institute for Health Research Biomedical Research Centre, Oxford, John Fell Oxford University Press Research Fund, Cancer Research UK (grant number C5255/A18085) through the Cancer Research UK Oxford Centre, and the Oxford Wellcome Institutional Strategic Support Fund (204826/Z/16/Z) during the conduct of the study, is an unpaid director of QResearch, a not-for-profit organisation which is a partnership between the University of Oxford and EMIS Health who supply the QResearch database used for this work, and is a founder and shareholder of ClinRisk Ltd and was its medical director until 31 May 2019; ClinRisk produces open and closed source software to implement clinical risk algorithms (outside this work) into clinical computer systems; CC reports receiving personal fees from ClinRisk, outside this work; AH is a member of the New and Emerging Respiratory Virus Threats Advisory Group; PJ was employed by NHS England during the conduct of the study and has received grants from Epizyme and Janssen and personal fees from Takeda, Bristol-Myers-Squibb, Novartis, Celgene, Boehringer Ingelheim, Kite Therapeutics, Genmab, and Incyte, all outside the submitted work; AKC has previously received personal fees from Huma Therapeutics, outside of the scope of the submitted work; RL has received grants from Health Data Research UK outside the submitted work; AS has received grants from the Medical Research Council (MRC) and Health Data Research UK during the conduct of the study; CS has received grants from the DHSC National Institute of Health Research UK, MRC UK, and the Health Protection Unit in Emerging and Zoonotic Infections (University of Liverpool) during the conduct of the study and is a minority owner in Integrum Scientific LLC (Greensboro, NC, USA) outside of the submitted work; KK has received grants from NIHR, is the national lead for ethnicity and diversity for the National Institute for Health Applied Research Collaborations, is director of the University of Leicester Centre for Black Minority Ethnic Health, was a steering group member of the Risk reduction Framework for NHS staff (chair) and for Adult care Staff, is a member of Independent SAGE, and is supported by the NIHR Applied Research Collaboration East Midlands (ARC EM) and the NIHR Leicester Biomedical Research Centre (BRC); RHK was supported by a UKRI Future Leaders Fellowship (MR/S017968/1); KDO was supported by a grant from the Alan Turing Institute Health Programme (EP/T001569/1); no other relationships or activities that could appear to have influenced the submitted work. The views expressed are those of the author(s) and not necessarily those of the NIHR, the NHS, or the Department of Health and Social Care.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center Global map. 2020. https://coronavirus.jhu.edu/map.html.
-
- Davies NG, Kucharski AJ, Eggo RM, Gimma A, Edmunds WJ, Centre for the Mathematical Modelling of Infectious Diseases COVID-19 working group Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: a modelling study. Lancet Public Health 2020;5:e375-85. 10.1016/S2468-2667(20)30133-X - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous