

(Rad 8)Caffeine prophylaxis to improve intermittent hypoxaemia in infants born late preterm: a randomised controlled dosage trial (Latte Dosage Trial)
- PMID: 33082191
- PMCID: PMC7577061
- DOI: 10.1136/bmjopen-2020-038271
(Rad 8)Caffeine prophylaxis to improve intermittent hypoxaemia in infants born late preterm: a randomised controlled dosage trial (Latte Dosage Trial)
Erratum in
-
Correction: (Rad 8)Caffeine prophylaxis to improve intermittent hypoxaemia in infants born late preterm: a randomised controlled dosage trial (Latte Dosage Trial).BMJ Open. 2020 Nov 6;10(11):1. doi: 10.1136/bmjopen-2020-038271corr1. BMJ Open. 2020. PMID: 33158841 Free PMC article. No abstract available.
Abstract
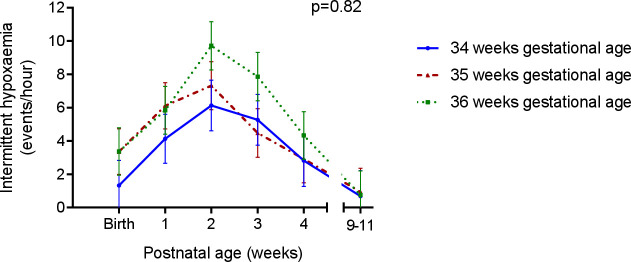
Introduction: Infants born late preterm (34+0 to 36+6 weeks' gestational age) have frequent episodes of intermittent hypoxaemia compared with term infants. Caffeine citrate reduces apnoea and intermittent hypoxaemia and improves long-term neurodevelopmental outcomes in infants born very preterm and may have similar effects in late preterm infants. Clearance of caffeine citrate increases with gestational age and late preterm infants are likely to need a higher dose than very preterm infants. Our aim is to determine the most effective and best-tolerated dose of caffeine citrate to reduce transient intermittent hypoxaemia events in late preterm infants.
Methods and analysis: A phase IIB, double-blind, five-arm, parallel, randomised controlled trial to compare the effect of four doses of oral caffeine citrate versus placebo on the frequency of intermittent hypoxaemia. Late preterm infants will be enrolled within 72 hours of birth and randomised to receive 5, 10, 15 or 20 mg/kg/day caffeine citrate or matching placebo daily until term corrected age. The frequency of intermittent hypoxaemia (events/hour where oxygen saturation concentration is ≥10% below baseline for ≤2 min) will be assessed with overnight oximetry at baseline, 2 weeks after randomisation (primary outcome) and at term corrected age. Growth will be measured at these timepoints, and effects on feeding and sleeping will be assessed by parental report. Data will be analysed using generalised linear mixed models.
Ethics and dissemination: This trial has been approved by the Health and Disability Ethics Committees of New Zealand (reference 18/NTA/129) and the local institutional research review committees. Findings will be disseminated to peer-reviewed journals to clinicians and researchers at local and international conferences and to the public. The findings of the trial will inform the design of a large multicentre trial of prophylactic caffeine in late preterm infants, by indicating the most appropriate dose to use and providing information on feasibility.
Trial registration number: ACTRN12618001745235; Pre-results.
Keywords: clinical pharmacology; neonatology; paediatric thoracic medicine.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Caffeine to prevent intermittent hypoxaemia in late preterm infants: randomised controlled dosage trial.Arch Dis Child Fetal Neonatal Ed. 2023 Mar;108(2):106-113. doi: 10.1136/archdischild-2022-324010. Epub 2022 Aug 29. Arch Dis Child Fetal Neonatal Ed. 2023. PMID: 36038256 Free PMC article. Clinical Trial.
-
Multicentre, randomised trial of preterm infants receiving caffeine and less invasive surfactant administration compared with caffeine and early continuous positive airway pressure (CaLI trial): study protocol.BMJ Open. 2021 Jan 22;11(1):e038343. doi: 10.1136/bmjopen-2020-038343. BMJ Open. 2021. PMID: 33483435 Free PMC article.
-
The effect of an additional pre-extubational loading dose of caffeine citrate on mechanically ventilated preterm infants (NEOKOFF trial): Study protocol for a multicenter randomized clinical trial.PLoS One. 2025 Jan 13;20(1):e0315856. doi: 10.1371/journal.pone.0315856. eCollection 2025. PLoS One. 2025. PMID: 39804861 Free PMC article.
-
Caffeine citrate: a review of its use in apnoea of prematurity.Paediatr Drugs. 2001;3(1):61-79. doi: 10.2165/00128072-200103010-00005. Paediatr Drugs. 2001. PMID: 11220405 Review.
-
Ontogeny of autonomic regulation in late preterm infants born at 34-37 weeks postmenstrual age.Semin Perinatol. 2006 Apr;30(2):73-6. doi: 10.1053/j.semperi.2006.02.005. Semin Perinatol. 2006. PMID: 16731280 Review.
Cited by
-
Caffeine dosing regimens in preterm infants with or at risk for apnea of prematurity.Cochrane Database Syst Rev. 2023 Apr 11;4(4):CD013873. doi: 10.1002/14651858.CD013873.pub2. Cochrane Database Syst Rev. 2023. PMID: 37040532 Free PMC article. Review.
-
Methylxanthine for the prevention and treatment of apnea in preterm infants.Cochrane Database Syst Rev. 2023 Oct 31;10(10):CD013830. doi: 10.1002/14651858.CD013830.pub2. Cochrane Database Syst Rev. 2023. PMID: 37905735 Free PMC article.
-
Caffeine to prevent intermittent hypoxaemia in late preterm infants: randomised controlled dosage trial.Arch Dis Child Fetal Neonatal Ed. 2023 Mar;108(2):106-113. doi: 10.1136/archdischild-2022-324010. Epub 2022 Aug 29. Arch Dis Child Fetal Neonatal Ed. 2023. PMID: 36038256 Free PMC article. Clinical Trial.
References
-
- Ministry of Health Report on Maternity 2017 - tables. Wellington, 2019. Available: https://www.health.govt.nz/publication/report-maternity-2017 [Accessed 8 Jul 2019].
-
- Martin JA, Hamilton BE, Osterman MJK, et al. . Births: final data for 2017, 2017. Available: https://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical