

Infection-Related Acute Care Events among Patients with Glomerular Disease
- PMID: 33082200
- PMCID: PMC7769021
- DOI: 10.2215/CJN.05900420
Infection-Related Acute Care Events among Patients with Glomerular Disease
Erratum in
-
Correction: Infection-Related Acute Care Events among Patients with Glomerular Disease.Clin J Am Soc Nephrol. 2021 Mar 8;16(3):456-457. doi: 10.2215/CJN.00550121. Clin J Am Soc Nephrol. 2021. PMID: 33648975 Free PMC article. No abstract available.
Abstract
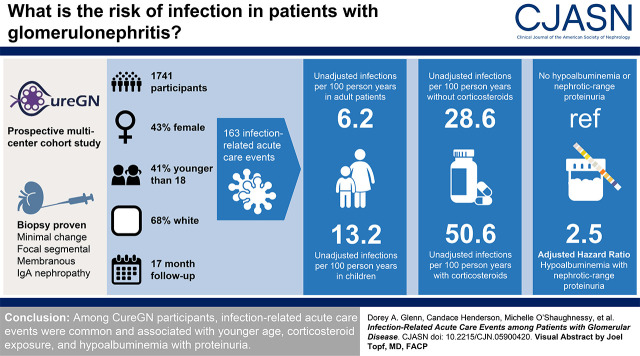
Background and objectives: Infections contribute to patient morbidity and mortality in glomerular disease. We sought to describe the incidence of, and identify risk factors for, infection-related acute care events among Cure Glomerulonephropathy Network (CureGN) study participants.
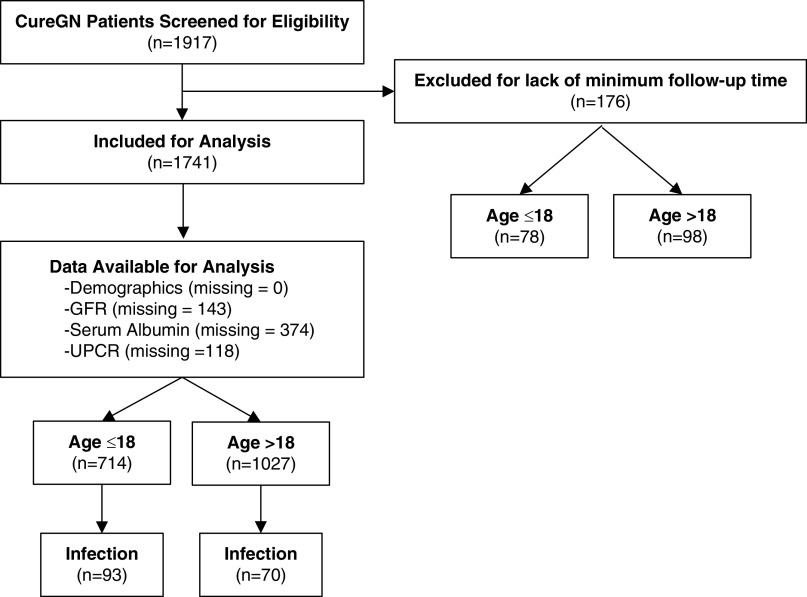
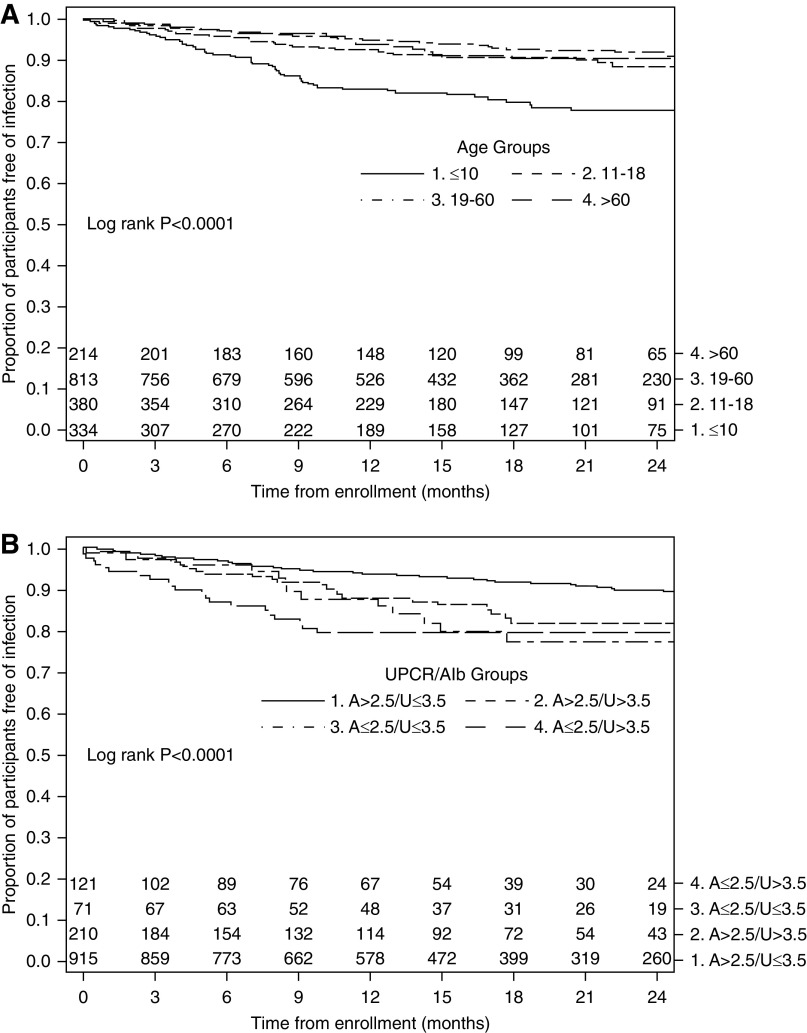
Design, setting, participants, & measurements: CureGN is a prospective, multicenter, cohort study of children and adults with biopsy sample-proven minimal change disease, FSGS, membranous nephropathy, or IgA nephropathy/vasculitis. Risk factors for time to first infection-related acute care events (hospitalization or emergency department visit) were identified using multivariable Cox proportional hazards regression.
Results: Of 1741 participants (43% female, 41% <18 years, 68% White), 163 (9%) experienced infection-related acute care events over a median follow-up of 17 months (interquartile range, 9-26 months). Unadjusted incidence rates of infection-related acute care events were 13.2 and 6.2 events per 100 person-years among pediatric and adult participants, respectively. Among participants with versus without corticosteroid exposure at enrollment, unadjusted incidence rates were 50.6 and 28.6 per 100 person-years, respectively, during the first year of follow-up (adjusted hazard ratio for time to first infection, 1.31; 95% CI, 0.89 to 1.93), and 4.1 and 1.1 per 100 person-years, respectively, after 1 year of follow-up (hazard ratio, 2.99; 95% CI, 1.54 to 5.79). Hypoalbuminemia combined with nephrotic-range proteinuria (serum albumin ≤2.5 g/dl and urinary protein-creatinine ratio >3.5 mg/mg), compared with serum albumin >2.5 g/dl and urinary protein-creatinine ratio ≤3.5 mg/mg, was associated with higher risk of time to first infection (adjusted hazard ratio, 2.49; 95% CI, 1.51 to 4.12).
Conclusions: Among CureGN participants, infection-related acute care events were common and associated with younger age, corticosteroid exposure, and hypoalbuminemia with proteinuria.
Keywords: acute care events; glomerular disease; hospitalization; immunosuppression; infection; kidney disease; nephrotic syndrome; pediatric nephrology.
Copyright © 2020 by the American Society of Nephrology.
Figures

Comment in
-
Correction: Infection-Related Acute Care Events among Patients with Glomerular Disease.Clin J Am Soc Nephrol. 2021 Mar 8;16(3):456-457. doi: 10.2215/CJN.00550121. Clin J Am Soc Nephrol. 2021. PMID: 33648975 Free PMC article. No abstract available.
References
-
- James MT, Quan H, Tonelli M, Manns BJ, Faris P, Laupland KB, Hemmelgarn BR; Alberta Kidney Disease Network : CKD and risk of hospitalization and death with pneumonia. Am J Kidney Dis 54: 24–32, 2009. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
