

Assessing Impact of HPV Vaccination on Cervical Cancer Incidence among Women Aged 15-29 Years in the United States, 1999-2017: An Ecologic Study
- PMID: 33082207
- PMCID: PMC7855406
- DOI: 10.1158/1055-9965.EPI-20-0846
Assessing Impact of HPV Vaccination on Cervical Cancer Incidence among Women Aged 15-29 Years in the United States, 1999-2017: An Ecologic Study
Abstract
Background: To date, the impact of the human papillomavirus (HPV) vaccine on invasive cervical cancers in the United States has not been documented due, in part, to the time needed for cancer to develop and to recent changes to cervical cancer screening guidelines and recommendations, which complicate data interpretation.
Methods: We examined incidence rates of cervical squamous cell carcinoma (SCC) and adenocarcinoma (AC) among women aged 15-29 years diagnosed during 1999-2017 using population-based cancer registry data covering 97.8% of the U.S.
Population: Trends were stratified by age and histology. The annual percent change in cervical cancer incidence per year was calculated using joinpoint regression.
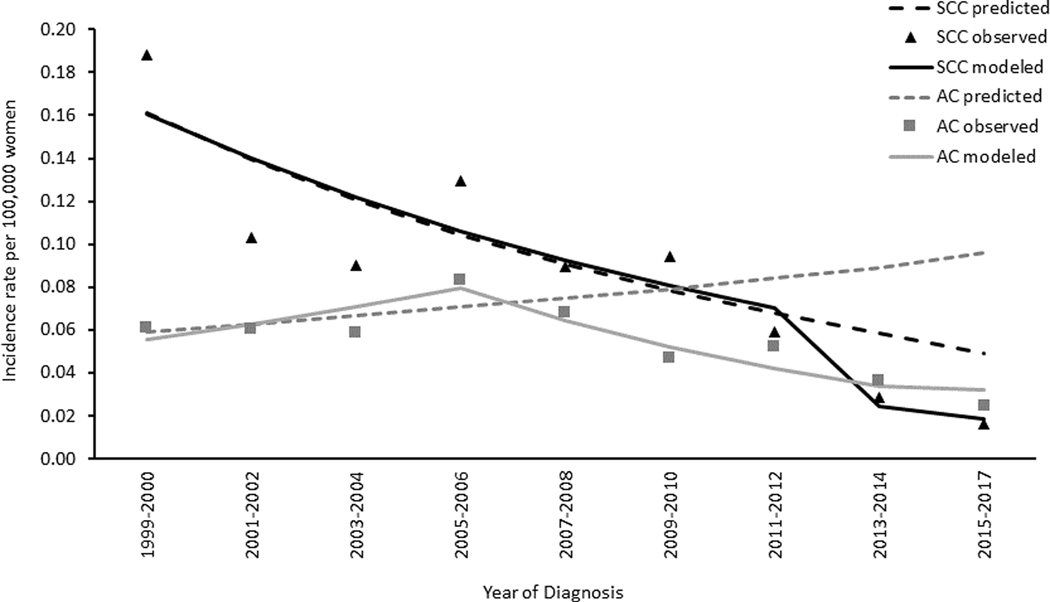
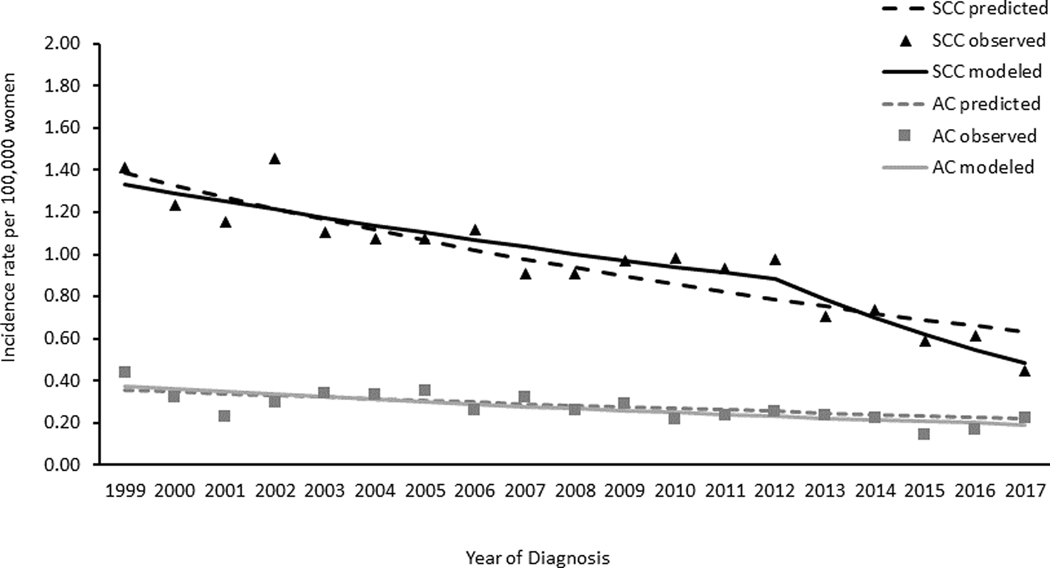
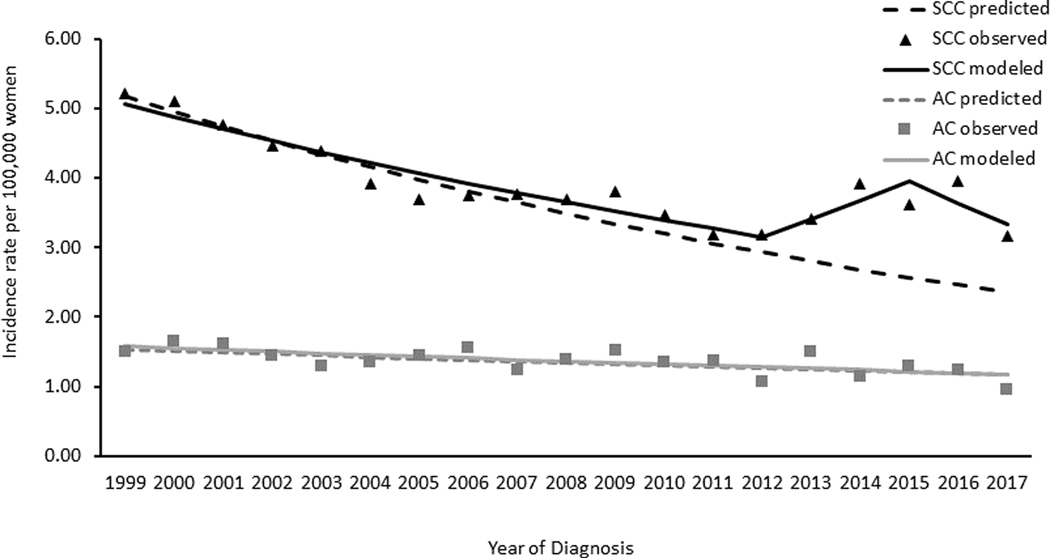
Results: During 1999-2017, SCC rates decreased 12.7% per year among women aged 15-20 years, 5.5% among women aged 21-24 years, and 2.3% among women aged 25-29 years. The declines in SCC rates were largest among women aged 15-20 years during 2010-2017, with a decrease of 22.5% per year. Overall, AC rates decreased 4.1% per year among women aged 15-20 years, 3.6% per year among women aged 21-24 years, and 1.6% per year among women aged 25-29 years. AC rates declined the most among women aged 15-20 years during 2006-2017, decreasing 9.4% per year.
Conclusions: Since HPV vaccine introduction, both SCC and AC incidence rates declined among women aged 15-20 years, a group not typically screened for cervical cancer, which may suggest HPV vaccine impact.
Impact: Timely vaccination and improved screening and follow-up among recommended age groups could result in further reductions in invasive cervical cancer.
©2020 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest
Figures
References
-
- Centers for Disease Control and Prevention. 2016. October 17. United States Cancer Statistics: Data Visualizations. <https://gis.cdc.gov/Cancer/USCS/DataViz.html>. Accessed 2019 October 17.
-
- Markowitz LE, Dunne EF, Saraiya M, Lawson HW, Chesson H, Unger ER. Quadrivalent human papillomavirus vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and reports : Morbidity and mortality weekly report Recommendations and reports 2007;56(Rr-2):1–24. - PubMed
-
- Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morbidity and mortality weekly report 2019;68(32):698–702 doi 10.15585/mmwr.mm6832a3. - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention. 2008. January 8 2008 Adolescent Human Papillomavirus (HPV) Vaccination Coverage Report. <https://www.cdc.gov/vaccines/imz-managers/coverage/teenvaxview/data-repo...>. Accessed 2020 January 8.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
