

Pain Relief after Surgical Decompression of the Distal Brachial Plexus
- PMID: 33082844
- PMCID: PMC7567639
- DOI: 10.1055/s-0040-1716718
Pain Relief after Surgical Decompression of the Distal Brachial Plexus
Abstract
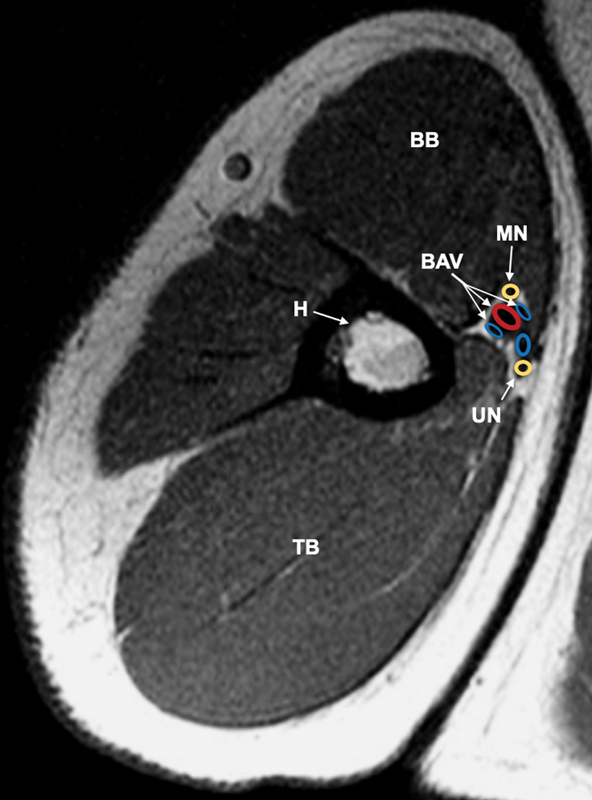
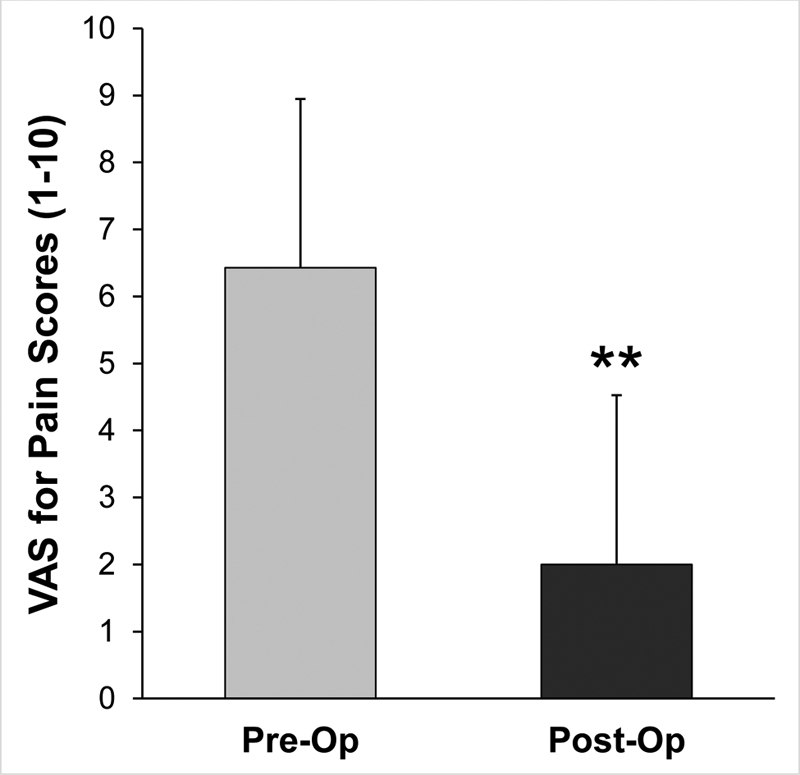
Background Brachial plexopathy causes pain and loss of function in the affected extremity. Entrapment of the brachial plexus terminal branches within the surrounding connective tissue, or medial brachial fascial compartment, may manifest in debilitating symptoms. Open fasciotomy and external neurolysis of the neurovascular bundle in the medial brachial fascial compartment were performed as a surgical treatment for pain and functional decline in the upper extremity. The aim of this study was to evaluate pain outcomes after surgery in patients diagnosed with brachial plexopathy. Methods We identified 21 patients who met inclusion criteria. Documents dated between 2005 and 2019 were reviewed from electronic medical records. Chart review was conducted to collect data on visual analog scale (VAS) for pain, Semmes-Weinstein monofilament test (SWMT), and Medical Research Council (MRC) scale for muscle strength. Pre- and postoperative data was obtained. A paired sample t -test was used to determine statistical significance of pain outcomes. Results Pain severity in the affected arm was significantly reduced after surgery (pre: 6.4 ± 2.5; post: 2.0 ± 2.5; p < 0.01). Additionally, there was an increased response to SWMT after the procedure. More patients achieved an MRC rating score ≥3 and ≥4 in elbow flexion after surgery. This may be indicative of improved sensory and motor function. Conclusion Open fasciotomy and external neurolysis at the medial brachial fascial compartment is an effective treatment for pain when nerve continuity is preserved. These benefits were evident in patients with a prolonged duration elapsed since injury onset.
Keywords: brachial plexopathy; brachial plexus; compression; entrapment; medial brachial fascial compartment; neuropathy; outcomes; pain; surgery.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures






References
-
- Faglioni W, Jr, Siqueira M G, Martins R S, Heise C O, Foroni L. The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Acta Neurochir (Wien) 2014;156(05):1025–1028. - PubMed
-
- Midha R.Epidemiology of brachial plexus injuries in a multitrauma population Neurosurgery 199740061182–1188., discussion 1188–1189 - PubMed
-
- Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986;3:S1–S226. - PubMed
-
- Institute of Medicine (U.S.) Committee on Advancing Pain Research, Care, and Education . Washington, DC: National Academies Press (U.S.); 2011. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. - PubMed
-
- Novak C B, Anastakis D J, Beaton D E, Katz J. Patient-reported outcome after peripheral nerve injury. J Hand Surg Am. 2009;34(02):281–287. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous