

Preoperative Risk Factors for Short-Term Postoperative Mortality of Acute Mesenteric Ischemia after Laparotomy: A Systematic Review and Meta-Analysis
- PMID: 33083058
- PMCID: PMC7556094
- DOI: 10.1155/2020/1382475
Preoperative Risk Factors for Short-Term Postoperative Mortality of Acute Mesenteric Ischemia after Laparotomy: A Systematic Review and Meta-Analysis
Abstract
Objective: Our objective was to comprehensively present the evidence of preoperative risk factors for short-term postoperative mortality of acute mesenteric ischemia after laparotomy.
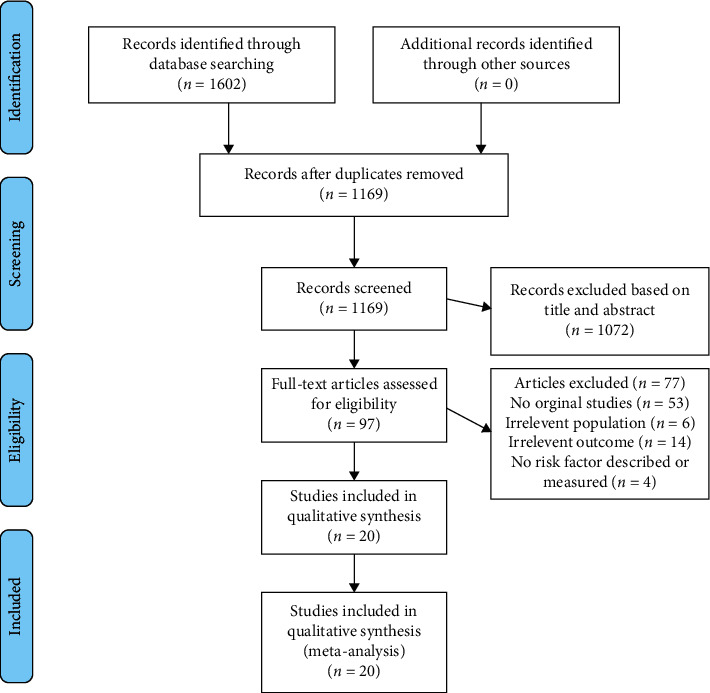
Methods: PubMed, Embase, and Google Scholar were searched from January 2000 to January 2020. Studies evaluating the postoperative risk factors for short-term postoperative mortality of acute mesenteric ischemia after laparotomy were included. The outcome extracted were patients' demographics, medical history, and preoperative laboratory tests.
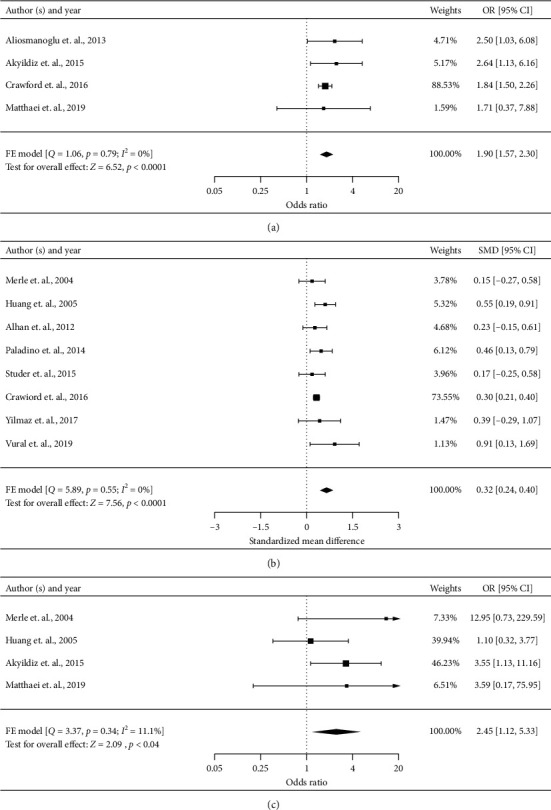
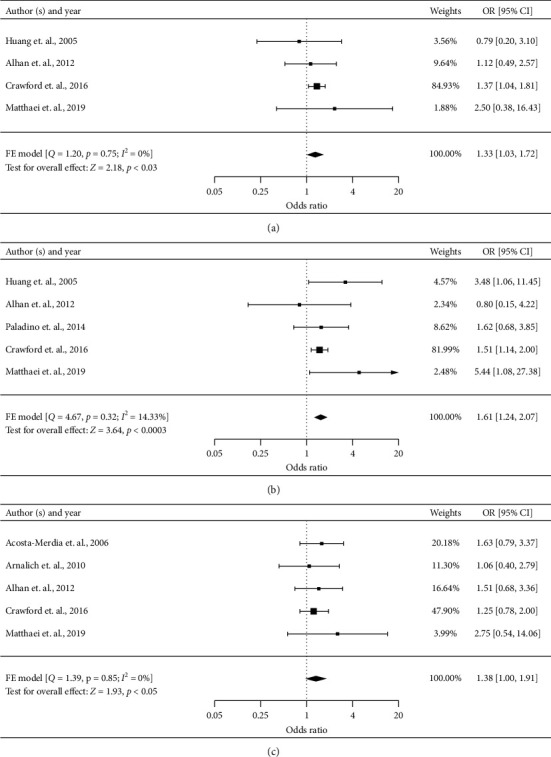
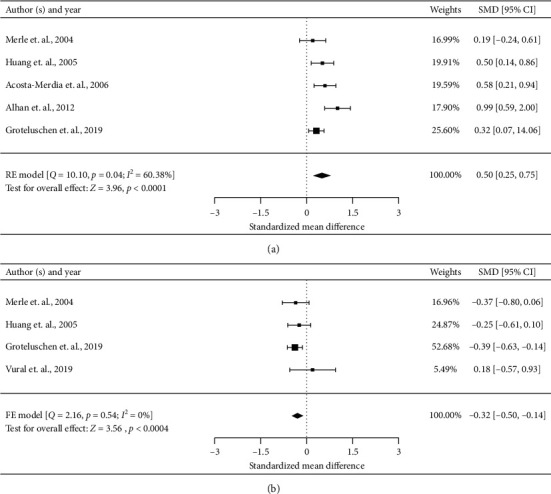
Results: Twenty studies (5011 patients) met the inclusion criteria. Studies were of high quality, with a median Newcastle-Ottawa Scale Score of 7. Summary short-term postoperative mortality was 44.38% (range, 18.80%-67.80%). Across included studies, 49 potential risk factors were examined, at least two studies. Meta-analysis of predictors based on more than three studies identified the following preoperative risk factors for higher short-term postoperative mortality risk: old age (odds ratio [OR], 1.90, 95% confidence interval [CI], 1.57-2.30), arterial occlusive mesenteric ischemia versus mesenteric venous thrombosis (OR, 2.45, 95% CI 1.12-5.33), heart failure (OR 1.33, 95% CI 1.03-1.72), renal disorders (OR 1.61, 95% CI 1.24-2.07), and peripheral vascular disease (OR 1.38, 95% CI 1.00-1.91). Nonsurvivors were older (standardized mean difference [SMD], 0.32, 95% CI 0.24-0.40), had higher creatinine levels (SMD 0.50, 95% CI 0.25-0.75), and had lower platelet counts (SMD -0.32, 95% CI -0.50 to -0.14).
Conclusion: The short-term postoperative mortality of acute mesenteric ischemia who underwent laparotomy is still high. A better understanding of these risk factors may help in the early identification of high-risk patients, optimization of surgical procedure, and improvement of perioperative management.
Copyright © 2020 Wenhan Wu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Fenestrated endovascular grafts for the repair of juxtarenal aortic aneurysms: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(4):1-51. Epub 2009 Jul 1. Ont Health Technol Assess Ser. 2009. PMID: 23074534 Free PMC article.
-
Incidence and outcomes of acute mesenteric ischaemia: a systematic review and meta-analysis.BMJ Open. 2022 Oct 25;12(10):e062846. doi: 10.1136/bmjopen-2022-062846. BMJ Open. 2022. PMID: 36283747 Free PMC article.
-
Is immediate imaging important in managing low back pain?J Athl Train. 2011 Jan-Feb;46(1):99-102. doi: 10.4085/1062-6050-46.1.99. J Athl Train. 2011. PMID: 21214357 Free PMC article.
-
Preoperative risk factors for 90-day postoperative mortality outcome in patients with non-occlusive mesenteric ischemia.Langenbecks Arch Surg. 2024 Jul 2;409(1):201. doi: 10.1007/s00423-024-03391-z. Langenbecks Arch Surg. 2024. PMID: 38954011
-
Contemporary Management of Acute Mesenteric Ischemia in the Endovascular Era.Vasc Endovascular Surg. 2019 Jan;53(1):42-50. doi: 10.1177/1538574418805228. Epub 2018 Oct 25. Vasc Endovascular Surg. 2019. PMID: 30360689 Review.
Cited by
-
Mortality Prediction Model before Surgery for Acute Mesenteric Infarction: A Population-Based Study.J Clin Med. 2022 Oct 8;11(19):5937. doi: 10.3390/jcm11195937. J Clin Med. 2022. PMID: 36233806 Free PMC article.
-
Results after intraoperative open and endovascular revascularization of acute mesenteric ischemia requiring a laparotomy.Langenbecks Arch Surg. 2023 Aug 10;408(1):303. doi: 10.1007/s00423-023-03035-8. Langenbecks Arch Surg. 2023. PMID: 37561214 Free PMC article.
-
Acute Mesenteric Ischemia: Preexisting Comorbidity Determines Short-Term Outcome and Quality of Life in Long-Term Survivors.Visc Med. 2022 Dec;38(6):393-399. doi: 10.1159/000526921. Epub 2022 Nov 24. Visc Med. 2022. PMID: 36589248 Free PMC article.
-
Factors that may affect the outcome of acute occlusive mesenteric ischemia. A single-center study.BMC Surg. 2024 Jan 13;24(1):21. doi: 10.1186/s12893-024-02310-9. BMC Surg. 2024. PMID: 38218808 Free PMC article.
-
A Comprehensive Way to Access Hospital Death Prediction Model for Acute Mesenteric Ischemia: A Combination of Traditional Statistics and Machine Learning.Int J Gen Med. 2021 Feb 25;14:591-602. doi: 10.2147/IJGM.S300492. eCollection 2021. Int J Gen Med. 2021. PMID: 33658832 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
