

Feasibility and acceptability of an online response inhibition cognitive training program for youth with Williams syndrome
- PMID: 33083211
- PMCID: PMC7560495
- DOI: 10.1016/bs.irrdd.2020.09.002
Feasibility and acceptability of an online response inhibition cognitive training program for youth with Williams syndrome
Abstract
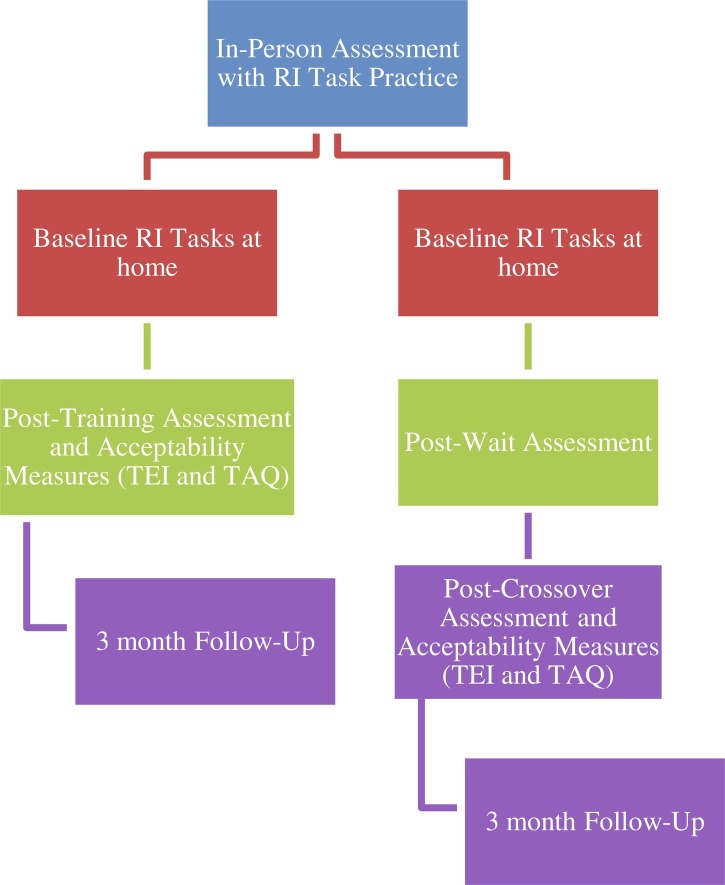
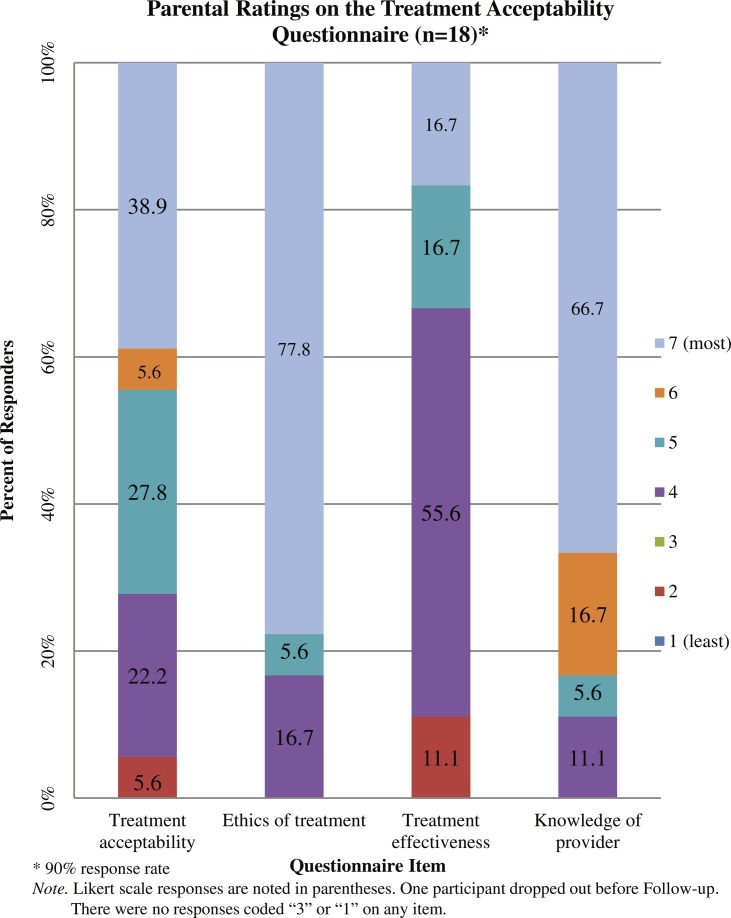
Williams syndrome (WS) is a genetic neurodevelopmental disorder often accompanied by inhibitory difficulties. Online cognitive training programs show promise for improving cognitive functions. No such interventions have been developed for individuals with WS, but to explore the practicality of large-scale online cognitive training for this population, we must first investigate whether families of those with WS find these programs feasible and acceptable. Twenty individuals aged 10-17 years with WS, along with parents, participated in a pilot online cognitive training program supervised in real time using videoconference software. We evaluated the feasibility and acceptability of this response inhibition training using three parent questionnaires. Descriptive data are reported for the measures of feasibility and acceptability. Overall, the online procedures received a positive reaction from families. Parents were likely to recommend the study to others. They indicated training was ethical and acceptable despite feeling neutral about effectiveness. The frequency and duration of sessions were acceptable to families (two 20-to-30-min sessions per week; 10 sessions total). Families provided feedback and offered suggestions for improvement, such as more flexibility in scheduling and decreasing time spent in review of procedures.
Keywords: Acceptability; Cognitive training; Feasibility; Internet-delivered training; Response inhibition; Williams syndrome.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures

References
-
- Baer R.A., Nietzel M.T. Cognitive and behavioral treatment of impulsivity in children: A meta-analytic review of the outcome literature. Journal of Clinical Child Psychology. 1991;20(4):400–412. doi: 10.1207/s15374424jccp2004_9. - DOI
-
- Botella C., Serrano B., Baños R.M., Garcia-Palacios A. Virtual reality exposure-based therapy for the treatment of post-traumatic stress disorder: A review of its efficacy, the adequacy of the treatment protocol, and its acceptability. Neuropsychiatric Disease and Treatment. 2015;11:2533–2545. doi: 10.2147/NDT.S89542. - DOI - PMC - PubMed
Further reading
LinkOut - more resources
Full Text Sources