

Localized primary gastric amyloidosis: Three case reports
- PMID: 33083432
- PMCID: PMC7559672
- DOI: 10.12998/wjcc.v8.i19.4667
Localized primary gastric amyloidosis: Three case reports
Abstract
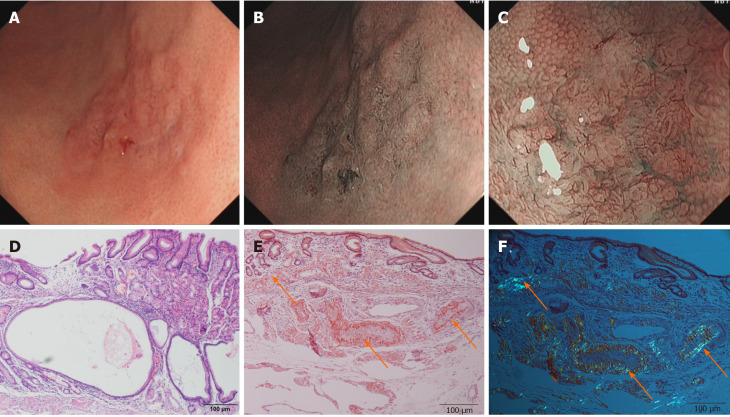
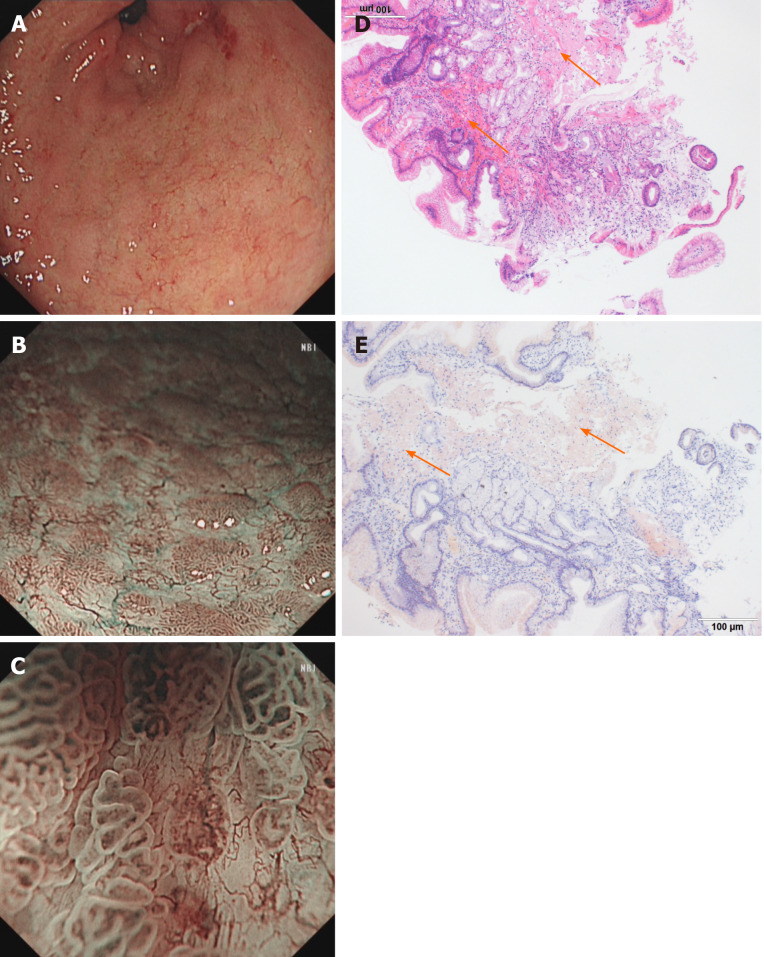
Background: Localized primary gastric amyloidosis is a rare disorder characterized by the extracellular deposition of insoluble fibrillary protein in the stomach and can mimic various diseases on endoscopic examination, including gastrointestinal stromal tumors, gastric cancer and ulcers.
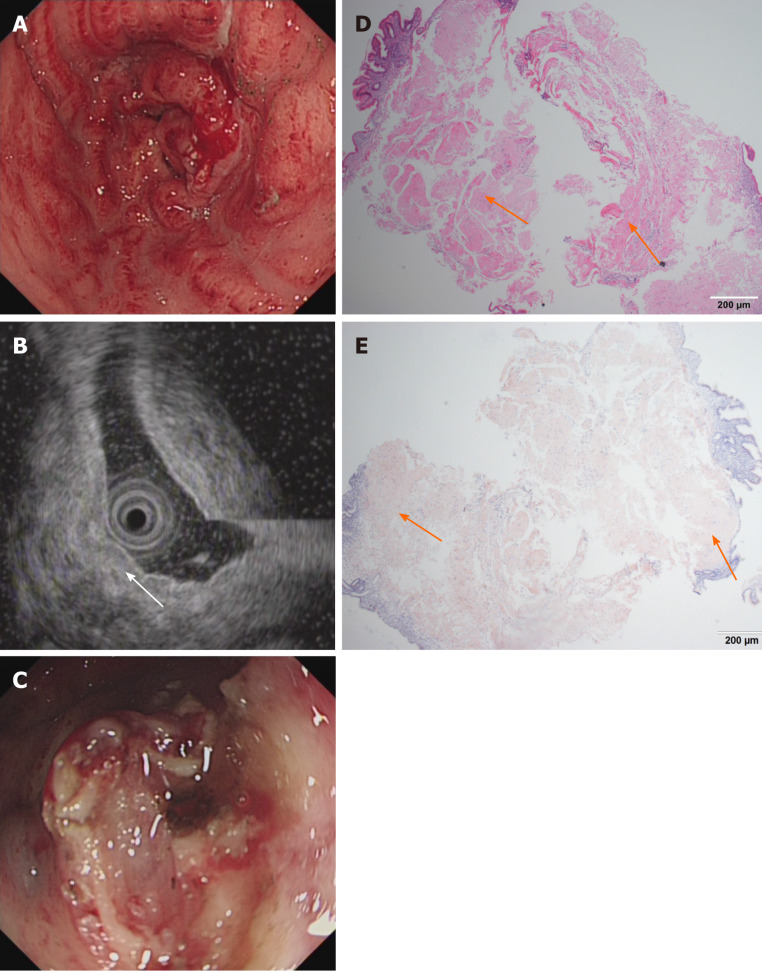
Case summaries: Here, we report a series of three cases of localized gastric amyloidosis mimicking gastric mucosa-associated lymphoid tissue (MALT) lymphoma on endoscopic examination that were evaluated over the past ten years in our hospital. The different detection times of this rare disease resulted in three completely different outcomes, indicating the strong importance of early detection, diagnosis and treatment. The difficulties encountered in making an accurate diagnosis and differential diagnosis are highlighted, and this report provides clinical experience for the diagnosis of localized primary gastric amyloidosis.
Conclusion: Localized gastric amyloidosis is a rare metabolic disease that resembles MALT lymphoma. Early detection, diagnosis and treatment of localized gastric amyloidosis result in an excellent prognosis.
Keywords: A case series study; Case report; Different outcomes; Localized gastric amyloidosis; Mucosa-associated lymphoid tissue lymphoma; Rare disease.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest.
Figures
Similar articles
-
A spectrum of Thymic mucosa-associated lymphoid tissue lymphoma and Thymic amyloidosis in the patient with Auto immune disease: a case series.Mediastinum. 2021 Jun 25;5:12. doi: 10.21037/med-20-68. eCollection 2021. Mediastinum. 2021. PMID: 35118318 Free PMC article.
-
[Gastric amyloidosis mimicking malignancy. A case report].Ann Chir. 2006 Oct;131(8):455-8. doi: 10.1016/j.anchir.2006.01.001. Epub 2006 Jan 23. Ann Chir. 2006. PMID: 16510115 French.
-
Localized primary amyloidosis of the stomach presenting with gastric hemorrhage.Acta Med Scand. 1987;221(1):115-9. doi: 10.1111/j.0954-6820.1987.tb01252.x. Acta Med Scand. 1987. PMID: 3494384
-
Primary localized gastric amyloidosis: A scoping review of the literature from clinical presentations to prognosis.World J Gastroenterol. 2021 Mar 28;27(12):1132-1148. doi: 10.3748/wjg.v27.i12.1132. World J Gastroenterol. 2021. PMID: 33828390 Free PMC article.
-
Localized amyloidosis of the stomach mimicking a superficial gastric cancer.Clin J Gastroenterol. 2016 Jun;9(3):109-13. doi: 10.1007/s12328-016-0651-x. Epub 2016 May 12. Clin J Gastroenterol. 2016. PMID: 27170299 Review.
Cited by
-
Gastrointestinal amyloidosis in a 50-year-old patient with miliary tuberculosis: A case report.Clin Case Rep. 2024 May 24;12(6):e8978. doi: 10.1002/ccr3.8978. eCollection 2024 Jun. Clin Case Rep. 2024. PMID: 38799515 Free PMC article.
-
Gastroduodenal amyloidosis: a case report and review of literature.J Surg Case Rep. 2021 Apr 22;2021(4):rjab093. doi: 10.1093/jscr/rjab093. eCollection 2021 Apr. J Surg Case Rep. 2021. PMID: 33936585 Free PMC article.
-
Pseudotumoral Amyloidosis Presentation With Upper Digestive Bleeding.Cureus. 2023 May 16;15(5):e39094. doi: 10.7759/cureus.39094. eCollection 2023 May. Cureus. 2023. PMID: 37332419 Free PMC article.
-
Localized light chain amyloidosis of the stomach that regressed after eradication of Helicobacter pylori over 15 years of follow-up: a case report and new hypothesis.Clin J Gastroenterol. 2025 Apr;18(2):269-277. doi: 10.1007/s12328-025-02097-z. Epub 2025 Jan 11. Clin J Gastroenterol. 2025. PMID: 39794679
-
Alpha-Fetoprotein-Producing Hepatoid Adenocarcinoma of the Stomach.J Med Cases. 2024 Oct;15(10):304-309. doi: 10.14740/jmc4263. Epub 2024 Sep 20. J Med Cases. 2024. PMID: 39328799 Free PMC article.
References
-
- Ebert EC, Nagar M. Gastrointestinal manifestations of amyloidosis. Am J Gastroenterol. 2008;103:776–787. - PubMed
-
- Ding Y, Li Y, Sun L. A Rare Case of Asymptomatic Primary Gastric Localized Amyloidosis. Clin Gastroenterol Hepatol. 2019;17:A41–A42. - PubMed
-
- Kinugasa H, Tanaka T, Okada H. Primary Localized Gastric Amyloidosis Mimicking a Submucosal Tumor-Like Gastrointestinal Tumor. Clin Gastroenterol Hepatol. 2020;18:e4. - PubMed
-
- Jin SZ, Qu B, Han MZ, Cheng YQ, Liang GY, Chu YJ, Zhu F, Liu BR. Endoscopic submucosal dissection combined with orally administered dimethyl sulfoxide for primary gastric localized amyloidosis. Clin Res Hepatol Gastroenterol. 2014;38:e79–e83. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
