

Age and environment-related differences in gait in healthy adults using wearables
- PMID: 33083562
- PMCID: PMC7528045
- DOI: 10.1038/s41746-020-00334-y
Age and environment-related differences in gait in healthy adults using wearables
Abstract
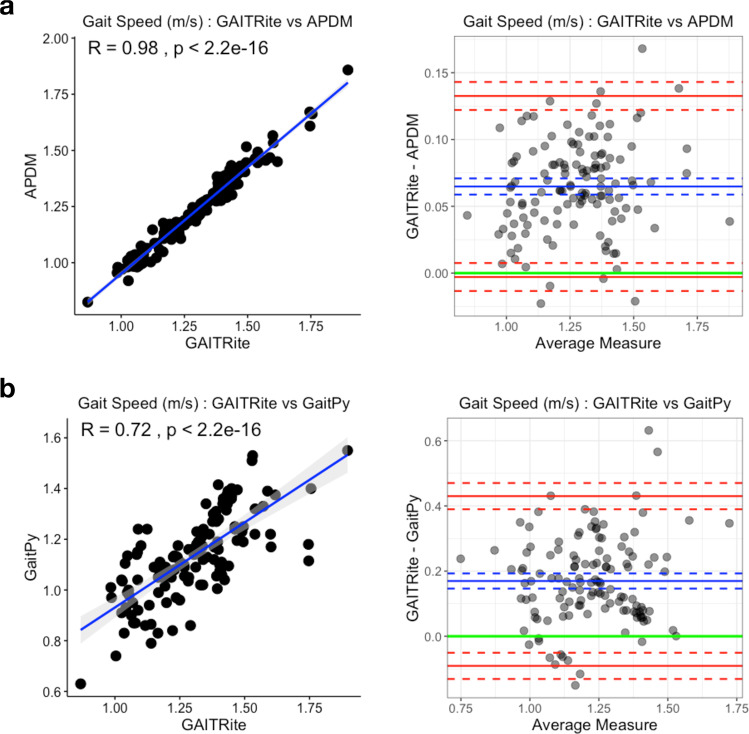
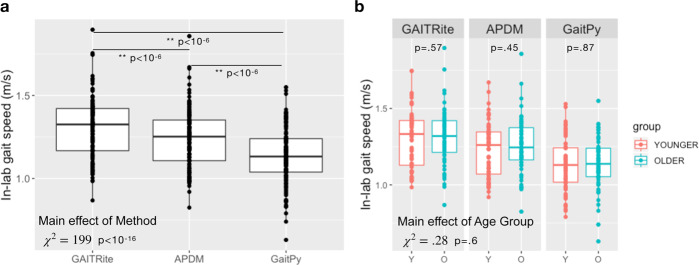
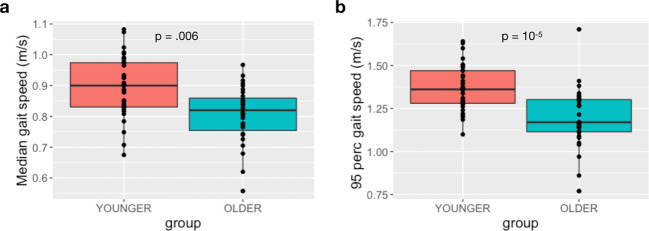
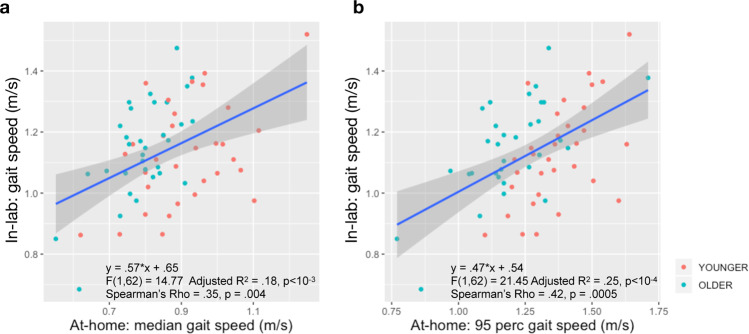
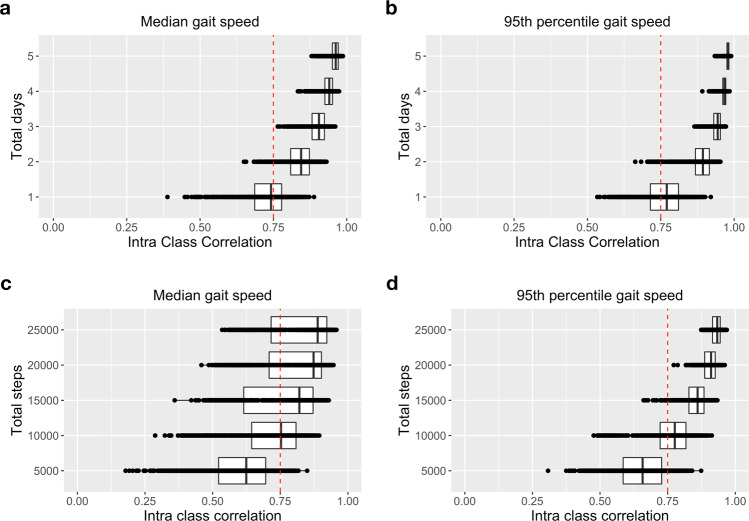
Technological advances in multimodal wearable and connected devices have enabled the measurement of human movement and physiology in naturalistic settings. The ability to collect continuous activity monitoring data with digital devices in real-world environments has opened unprecedented opportunity to establish clinical digital phenotypes across diseases. Many traditional assessments of physical function utilized in clinical trials are limited because they are episodic, therefore, cannot capture the day-to-day temporal fluctuations and longitudinal changes in activity that individuals experience. In order to understand the sensitivity of gait speed as a potential endpoint for clinical trials, we investigated the use of digital devices during traditional clinical assessments and in real-world environments in a group of healthy younger (n = 33, 18-40 years) and older (n = 32, 65-85 years) adults. We observed good agreement between gait speed estimated using a lumbar-mounted accelerometer and gold standard system during the performance of traditional gait assessment task in-lab, and saw discrepancies between in-lab and at-home gait speed. We found that gait speed estimated in-lab, with or without digital devices, failed to differentiate between the age groups, whereas gait speed derived during at-home monitoring was able to distinguish the age groups. Furthermore, we found that only three days of at-home monitoring was sufficient to reliably estimate gait speed in our population, and still capture age-related group differences. Our results suggest that gait speed derived from activities during daily life using data from wearable devices may have the potential to transform clinical trials by non-invasively and unobtrusively providing a more objective and naturalistic measure of functional ability.
Keywords: Biomedical engineering; Predictive markers; Quality of life.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsM.D.C., D.P., H.Z., T.A., A.K., A.M., K.R.A.V.D., V.R., C.D., X.C., M.S., S.P., and F.I.K. are current employees of Pfizer, Inc. M.C. was a former employee of Pfizer, Inc.
Figures
References
-
- Fritz S, Lusardi M. Whitepaper: "Walking Speed: the Sixth Vital Sign". J. Geriatr.Phys. Ther. 2009;32:2–5. - PubMed
-
- Hornyak V, Vanswearingen JM, Brach JS. Measurement of gait speed. Top. Geriatr. Rehabil. 2012;28:27–32.
-
- Peel NM, Kuys SS, Klein K. Gait speed as a measure in geriatric assessment in clinical settings: a systematic review. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012;68:39–46. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
