

Acute idiopathic blind spot enlargement syndrome following influenza vaccination
- PMID: 33083635
- PMCID: PMC7554322
- DOI: 10.1016/j.ajoc.2020.100949
Acute idiopathic blind spot enlargement syndrome following influenza vaccination
Abstract
Purpose: To report a case of acute idiopathic blind spot enlargement syndrome (AIBSES) following influenza vaccination.
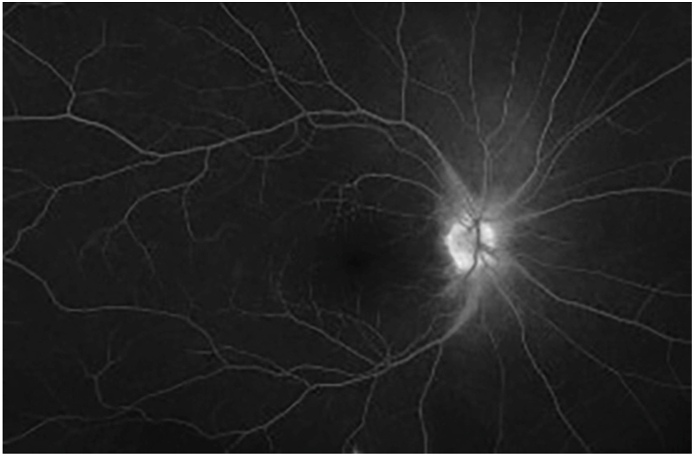
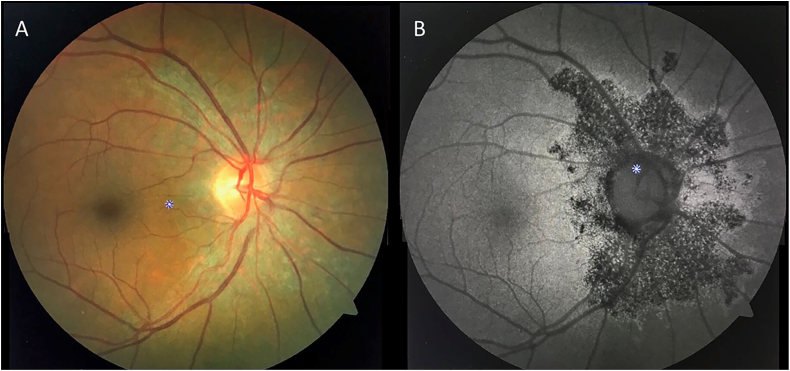
Observations: A 57-year old woman presented with a one-month history of photopsia, temporal visual field disturbance on the right eye, 11 days following the administration of the influenza virus vaccine. Visual acuity was 20/30, and color vision remained normal. Examination revealed mild venular dilation at the edge of the right optic disk and was otherwise unremarkable. Visual field testing revealed enlargement of the right physiological blind spot. Medical workup, including brain CT scan, brain MRI, RPR, Treponema pallidum antibodies, Chest X-Ray, ANA, and PPD testing, was found within normal limits. Ancillary testing was compatible with an assessment of AIBSES secondary to influenza virus vaccination.
Conclusions and importance: Although direct causation may not be absolutely established by a single report, our case suggests that the influenza virus vaccine may serve as an immunological trigger for some cases of AIBSES. Thoughtful vaccination history is of the utmost importance when evaluating patients with AIBSES, as it may help elucidate the underlying precipitating factor. To our knowledge, this is the first reported case of AIBSES following influenza virus vaccination.
Keywords: Acute blind spot enlargement syndrome; Influenza virus; Vaccination.
© 2020 The Authors.
Conflict of interest statement
No funding or grant support was provided for this report. The following authors have no financial disclosures: XQ, JO, CS, AO, JR. All authors attest that they meet the current ICMJE criteria for Authorship.
Figures



References
-
- Volpe N.J., Rizzo J.F., Lessell S. Acute idiopathic blind spot enlargement syndrome: a review of 27 new cases. Arch Ophthalmol. 2001;119(1):59–63. http://www.ncbi.nlm.nih.gov/pubmed/11146727 (Chicago, Ill 1960) Accessed June 18, 2019. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
