

A theoretical model for graft punch size calculations to prevent Descemet's membrane folds following deep anterior lamellar keratoplasty
- PMID: 33084812
- PMCID: PMC12289264
- DOI: 10.5935/0004-2749.20200077
A theoretical model for graft punch size calculations to prevent Descemet's membrane folds following deep anterior lamellar keratoplasty
Abstract
Purpose: The length of Descemet's membrane and donor graft sizes in deep anterior lamellar keratoplasty do not match in very steep corneas, which can lead to Descemet's membrane folds. The aim of this study is to establish a theoretical model for graft size calculations for deep anterior lamellar keratoplasty and evaluate its efficacy for preventing Descemet's membrane folds.
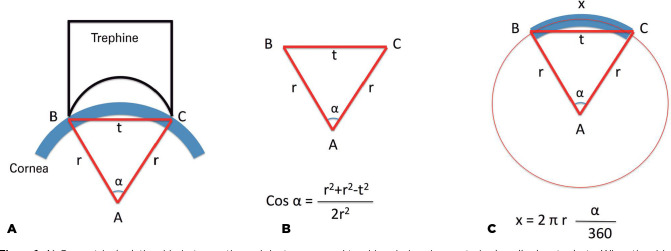
Methods: We calculated the arc diameter of the recipient bed by using the cosine formula and developed a table to aid surgeons in donor punch size selection. To test the usefulness of this formula, we evaluated the development of Descemet's membrane folds in keratoconus patients with very steep corneas (K >60 D). In group 1, deep anterior lamellar keratoplasty surgeries were performed using graft sizes that were determined based on our model (n=31). In group 2, graft sizes were determined based on the empirical judgment of the surgeon without any formal calculation (n=30).
Results: Our theoretical calculations demonstrated that the diameter of donor punch sizes needed to prevent Descemet's membrane fold increases when the cornea is steeper, or the trephine size is larger. We tested the efficacy of this model on the clinical outcome of deep anterior lamellar keratoplasty. The mean age (28.9 ± 10.1 years vs. 32.8 ± 8.3 years, p=0.11) and preoperative K1 (59.2 ± 9.3 D vs. 58.1 ± 9.4 D, p=0.67), K2 (66.2 ± 6.0 D vs. 65.7 ± 7.4 D, p=0.81), and Km values (62.1 ± 7.7 D vs. 61.8 ± 8.1 D, p=0.88) were similar between the two groups. Three patients developed Descemet's membrane folds in group 2, and none of the patients developed Descemet's membrane folds in group 1. These results supported our theo retical calculations.
Conclusion: Adjustment of donor graft size based on the calculated arc diameter of the recipient bed reduced the development of Descemet's membrane folds after deep anterior lamellar keratoplasty in steep corneas.
Objetivo: O comprimento da membrana de Descemet e o tamanho do enxerto doador na ceratoplastia lamelar anterior profunda não coincidem em córneas muito íngremes, o que pode levar às dobras da membrana de Descemet. O objetivo deste estudo é estabelecer um modelo teórico para cálculo do tamanho do enxerto para ceratoplastia lamelar anterior profunda e avaliar a sua eficácia na prevenção de dobras da membrana de Descemet.
Métodos: Calculamos o diâmetro do arco do leito receptor usando a fórmula do cosseno e desenvolvemos uma tabela para auxiliar os cirurgiões na seleção do tamanho da punção no doador. Para testar a utilidade dessa fórmula, avaliamos o desenvolvimento das dobras da membrana de Descemet em pacientes com ceratocone com córneas muito íngremes (K>60D). No grupo 1, foram realizadas cirurgias de ceratoplastia lamelar anterior profunda, utilizando tamanhos de enxerto que foram determinados com base em nosso modelo (n=31). No grupo 2, os tamanhos dos enxertos foram determinados com base no julgamento empírico do cirurgião sem qualquer cálculo formal (n=30).
Resultados: Nossos cálculos teóricos demonstraram que o diâmetro dos tamanhos da punção do doador necessários para evitar as dobras na membrana de Descemet aumenta quando a córnea é mais íngreme ou o tamanho da trefina é maior. Testamos a eficácia deste modelo no resultado clínico da ceratoplastia lamelar anterior profunda. A média de idade (28,9 ± 10,1 anos vs. 32,8 ± 8,3 anos, p=0,11) e K1 pré-operatório (59,2 ± 9,3 D vs. 58,1 ± 9,4 D, p=0,67), K2 (66,2 ± 6,0 D vs. 65,7 ± 7,4) D, p=0,81) e Km (62,1 ± 7,7 D vs. 61,8 ± 8,1 D, p=0,88) foram semelhantes entre os dois grupos. Três pacientes desenvolveram dobras na membrana de Descemet no grupo 2, e nenhum dos pacientes desenvolveu dobras na membrana de Descemet no grupo 1. Estes resultados apoiam nossos cálculos teóricos.
Conclusão: O ajuste do tamanho do enxerto doador com base no diâmetro do arco calculado do leito receptor reduziu o desenvolvimento das dobras na membrana de Descemet após ceratoplastia lamelar anterior profunda em córneas íngremes.
Conflict of interest statement
Figures

References
-
- Wagoner MD, Smith SD, Rademaker WJ, Mahmood MA. Penetrating keratoplasty vs. epikeratoplasty for the surgical treatment of keratoconus. J Refract Surg. 2001;17(2):138–146. - PubMed
-
- Pakrou N, Fung S, Selva D, Chehade M, Leibovitch I. Deep lamellar keratoplasty in the treatment of keratoconus. Ophthalmologica. 2006;220(3):164–169. - PubMed
-
- Fontana L, Parente G, Tassinari G. Clinical outcomes after deep anterior lamellar keratoplasty using the big-bubble technique in patients with keratoconus. Am J Ophthalmol. 2007;143(1):117–124. - PubMed
-
- Bahar I, Kaiserman I, Srinivasan S, Ya-Ping J, Slomovic AR, Rootman DS. Comparison of three different techniques of corneal transplantation for keratoconus. Am J Ophthalmol. 2008;146(6):905–12. e1. - PubMed
-
- Terry MA. The evolution of lamellar grafting techniques over twentyfive years. Cornea. 2000;19(5):611–616. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
