

Patient-Reported Outcomes of Robotic vs Laparoscopic Ventral Hernia Repair With Intraperitoneal Mesh: The PROVE-IT Randomized Clinical Trial
- PMID: 33084881
- PMCID: PMC7578919
- DOI: 10.1001/jamasurg.2020.4569
Patient-Reported Outcomes of Robotic vs Laparoscopic Ventral Hernia Repair With Intraperitoneal Mesh: The PROVE-IT Randomized Clinical Trial
Abstract
Importance: Despite rapid adoption of the robotic platform for ventral hernia repair with intraperitoneal mesh in the United States, there is no level I evidence comparing it with the traditional laparoscopic approach. This randomized clinical trial sought to demonstrate a clinical benefit to the robotic approach.
Objective: To determine whether robotic approach to ventral hernia repair with intraperitoneal mesh would result in less postoperative pain.
Design, setting, and participants: A registry-based, single-blinded, prospective randomized clinical trial at the Cleveland Clinic Center for Abdominal Core Health, Cleveland, Ohio, completed between September 2017 and January 2020, with a minimum follow-up duration of 30 days. Two surgeons at 1 academic tertiary care hospital. Patients with primary or incisional midline ventral hernias of an anticipated width of 7 cm or less presenting in the elective setting and able to tolerate a minimally invasive repair.
Interventions: Patients were randomized to a standardized laparoscopic or robotic ventral hernia repair with fascial closure and intraperitoneal mesh.
Main outcomes and measures: The trial was powered to detect a 30% difference in the Numerical Rating Scale (NRS-11) on the first postoperative day. Secondary end points included the Patient-Reported Outcomes Measurement Information System Pain Intensity short form (3a), hernia-specific quality of life, operative time, wound morbidity, recurrence, length of stay, and cost.
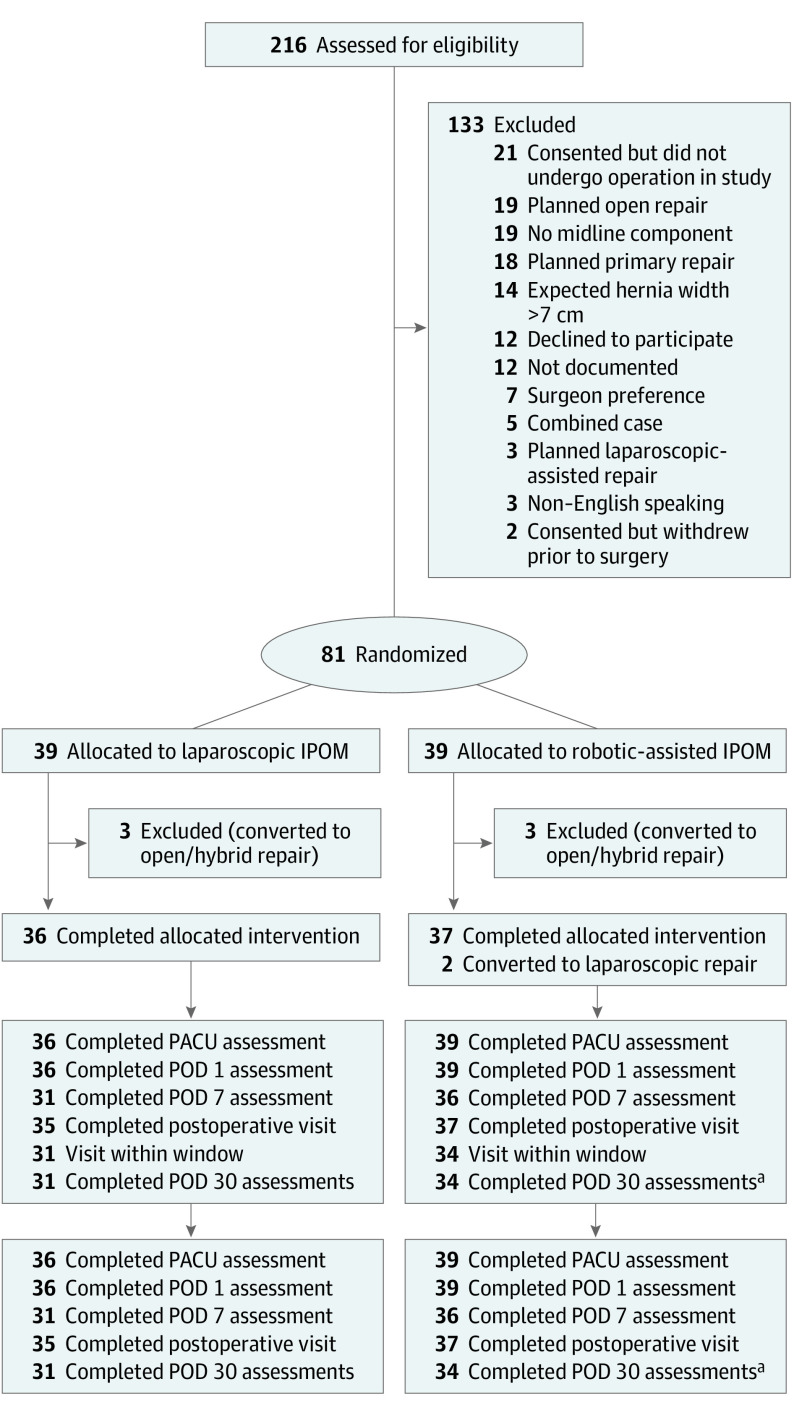
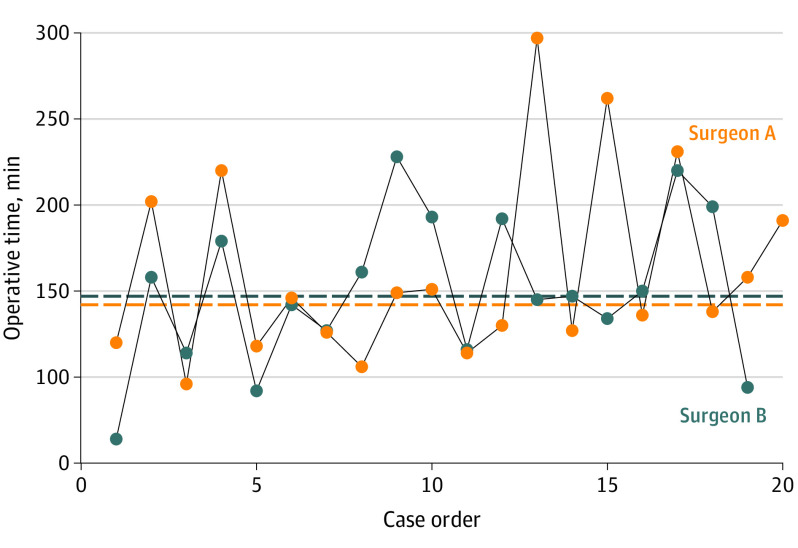
Results: Seventy-five patients completed their minimally invasive hernia repair: 36 laparoscopic and 39 robotic. Baseline demographics and hernia characteristics were comparable. Robotic operations had a longer median operative time (146 vs 94 minutes; P < .001). There were 2 visceral injuries in each cohort but no full-thickness enterotomies or unplanned reoperations. There were no significant differences in NRS-11 scores preoperatively or on postoperative days 0, 1, 7, or 30. Specifically, median NRS-11 scores on the first postoperative day were the same (5 vs 5; P = .61). Likewise, postoperative Patient-Reported Outcomes Measurement Information System 3a and hernia-specific quality-of-life scores, as well as length of stay and complication rates, were similar. The robotic platform adds cost (total cost ratio, 1.13 vs 0.97; P = .03), driven by the cost of additional operating room time (1.25 vs 0.85; P < .001).
Conclusions and relevance: Laparoscopic and robotic ventral hernia repair with intraperitoneal mesh have comparable outcomes. The increased operative time and proportional cost of the robotic approach are not offset by a measurable clinical benefit.
Trial registration: ClinicalTrials.gov Identifier: NCT03283982.
Conflict of interest statement
Figures
Comment in
-
The Robot in General Surgery-Change Is the Only Constant.JAMA Surg. 2021 Jan 1;156(1):30. doi: 10.1001/jamasurg.2020.4590. JAMA Surg. 2021. PMID: 33084850 No abstract available.
-
Does PROVE-IT Really Prove Anything of Value?JAMA Surg. 2021 Aug 1;156(8):797. doi: 10.1001/jamasurg.2021.0956. JAMA Surg. 2021. PMID: 33909011 No abstract available.
-
Does PROVE-IT Really Prove Anything of Value?-Reply.JAMA Surg. 2021 Aug 1;156(8):797-798. doi: 10.1001/jamasurg.2021.0957. JAMA Surg. 2021. PMID: 33909038 No abstract available.
References
-
- Carbonell AM, Warren JA, Prabhu AS, et al. Reducing length of stay using a robotic-assisted approach for retromuscular ventral hernia repair: a comparative analysis from the Americas Hernia Society Quality Collaborative. Ann Surg. 2018;267(2):210-217. doi: 10.1097/SLA.0000000000002244 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
