

An Analysis of 30-Day in-Hospital Trauma Mortality in Four Urban University Hospitals Using the Australia India Trauma Registry
- PMID: 33084947
- PMCID: PMC7773616
- DOI: 10.1007/s00268-020-05805-7
An Analysis of 30-Day in-Hospital Trauma Mortality in Four Urban University Hospitals Using the Australia India Trauma Registry
Abstract
Background: India has one-sixth (16%) of the world's population but more than one-fifth (21%) of the world's injury mortality. A trauma registry established by the Australia India Trauma Systems Collaboration (AITSC) Project was utilized to study 30-day in-hospital trauma mortality at high-volume Indian hospitals.
Methods: The AITSC Project collected data prospectively between April 2016 and March 2018 at four Indian university hospitals in New Delhi, Mumbai, and Ahmedabad. Patients admitted with an injury mechanism of road or rail-related injury, fall, assault, or burns were included. The associations between demographic, physiological on-admission vitals, and process-of-care parameters with early (0-24 h), delayed (1-7 days), and late (8-30 days) in-hospital trauma mortality were analyzed.
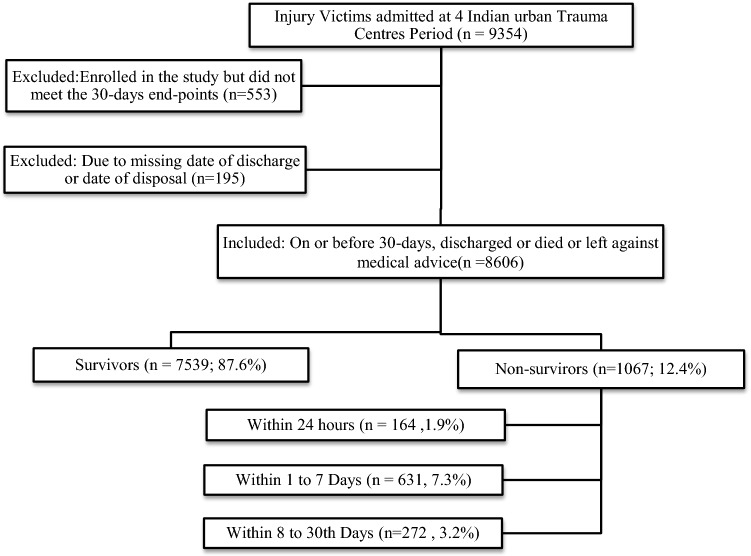
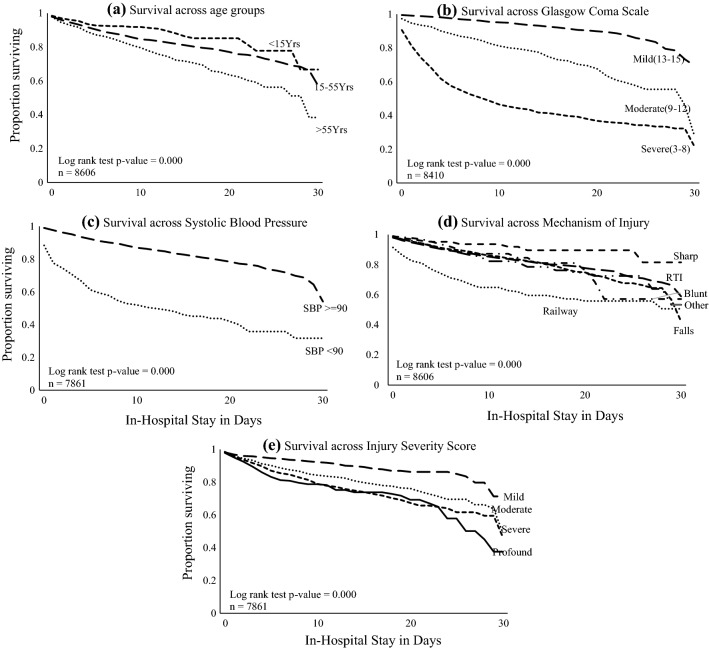
Results: Of 9354 patients in the AITSC registry, 8606 were subjected to analysis. The 30-day mortality was 12.4% among all trauma victims. Early (24-h) mortality was 1.9%, delayed (1-7 days) mortality was 7.3%, and late (8-30 days) mortality was 3.2%. Abnormal physiological parameters such as a low SBP, SpO2, and GCS and high HR and RR were observed among non-survivors. Early initiation of trauma assessment and monitoring on arrival was an important process of care indicator for predicting 30-day survival.
Conclusions: One in ten admitted trauma patients (12.4%) died in urban trauma centers in India. More than half of the trauma deaths were delayed, beyond 24 h but within one week following injury. On-admission physiological vital signs remain a valid predictor of early 24-h trauma mortality.
Conflict of interest statement
The authors have declared that no conflicts of interests exist.
Figures

References
-
- Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- WHO (2014) Injuries and violence: the facts 2014.
-
- WHO (2013) Global status report on road safety. Inj Prev 318. https://doi.org/https://www.who.int/violence_injury_prevention/road_safety_status/2013/e...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
