

Intraoral ultrasonography in the assessment of DOI in oral cavity squamous cell carcinoma: a comparison with magnetic resonance and histopathology
- PMID: 33084951
- PMCID: PMC8266699
- DOI: 10.1007/s00405-020-06421-w
Intraoral ultrasonography in the assessment of DOI in oral cavity squamous cell carcinoma: a comparison with magnetic resonance and histopathology
Abstract
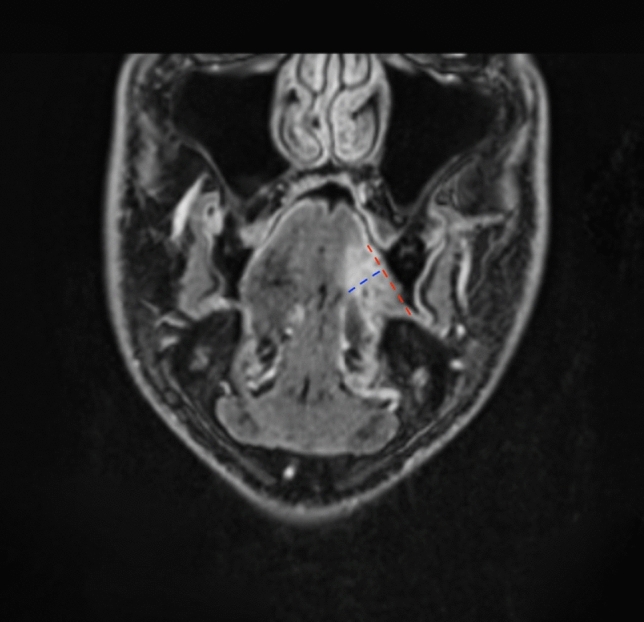
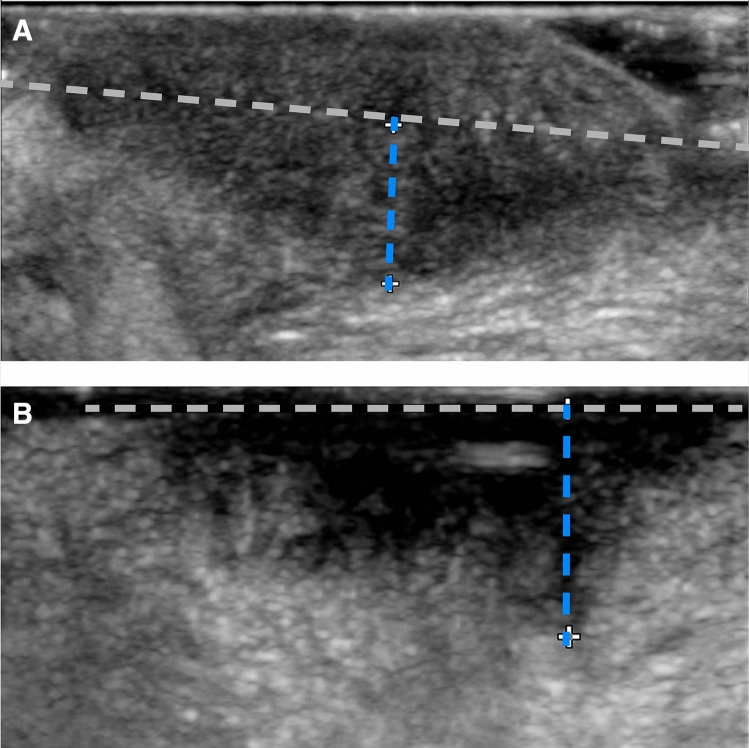
Objective: The first-line therapeutic approach for oral cavity squamous cell carcinoma (OCSCC) is complete surgical resection. Preoperative assessment of depth of invasion (cDOI) is crucial to plan the surgery. Magnetic resonance (MR) and intraoral ultrasonography (IOUS) have been shown to be useful tools for assessment of DOI. The present analysis investigates the accuracy of MR and IOUS in evaluating DOI in OCSCC compared to histological evaluation (pDOI).
Materials and methods: Forty-nine previously untreated patients with cT1-T3 OCSCC were reviewed. Nine patients were staged with MR alone, 10 with IOUS alone, and 30 with both MR and IOUS.
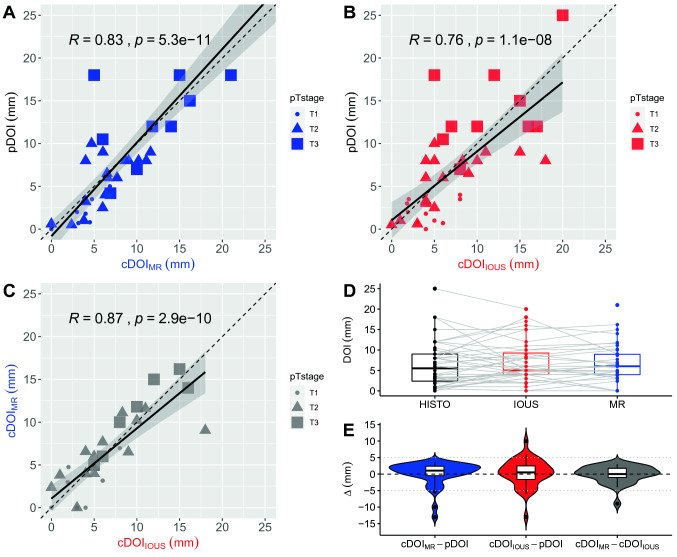
Results: Mean difference between cDOIMR and pDOI values of 0.2 mm (95% CI - 1.0-1.3 mm) and between cDOIIOUS and pDOI of 0.3 mm (95% CI - 1.0-1.6 mm). Spearman R between cDOIMR and pDOI was R = 0.83 and between cDOIIOUS and pDOI was R = 0.76. Both radiological techniques showed high performance for the correct identification, with the optimum cut-off of 5 mm, of patients with a pDOI ≥ 4 mm and amenable to a neck dissection, with an AUC of 0.92 and 0.82 for MR and IOUS, respectively.
Conclusion: Both examinations were valid approaches for preoperative determination of DOI in OCSCC, although with different cost-effectiveness profiles and indications.
Keywords: Depth of invasion; Head and neck; Magnetic resonance imaging; Mouth; Neoplasm; Ultrasonography.
Conflict of interest statement
The authors certify that they have no affiliation with or involvement in any organization or entity with any financial interest.
Figures

Similar articles
-
High-Frequency Intraoral Ultrasound for Preoperative Assessment of Depth of Invasion for Early Tongue Squamous Cell Carcinoma: Radiological-Pathological Correlations.Int J Environ Res Public Health. 2022 Nov 12;19(22):14900. doi: 10.3390/ijerph192214900. Int J Environ Res Public Health. 2022. PMID: 36429617 Free PMC article.
-
Punch Biopsy for Preoperative Depth of Invasion Assessment in Early Oral Tongue Squamous Cell Carcinoma: A Prospective Pilot Study.J Otolaryngol Head Neck Surg. 2025 Jan-Dec;54:19160216251321452. doi: 10.1177/19160216251321452. Epub 2025 Apr 1. J Otolaryngol Head Neck Surg. 2025. PMID: 40170359 Free PMC article.
-
Novel pathological predictive factors for extranodal extension in oral squamous cell carcinoma: a retrospective cohort study based on tumor budding, desmoplastic reaction, tumor-infiltrating lymphocytes, and depth of invasion.BMC Cancer. 2022 Apr 13;22(1):402. doi: 10.1186/s12885-022-09393-8. BMC Cancer. 2022. PMID: 35418058 Free PMC article.
-
Magnetic Resonance vs. Intraoral Ultrasonography in the Preoperative Assessment of Oral Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis.Front Oncol. 2020 Feb 4;9:1571. doi: 10.3389/fonc.2019.01571. eCollection 2019. Front Oncol. 2020. PMID: 32117789 Free PMC article.
-
Correlation between radiologic depth of invasion and pathologic depth of invasion in oral cavity squamous cell carcinoma: A systematic review and meta-analysis.Oral Oncol. 2023 Jan;136:106249. doi: 10.1016/j.oraloncology.2022.106249. Epub 2022 Nov 20. Oral Oncol. 2023. PMID: 36417807
Cited by
-
The Applications and Potential Developments of Ultrasound in Oral Cancer Management.Technol Cancer Res Treat. 2022 Jan-Dec;21:15330338221133216. doi: 10.1177/15330338221133216. Technol Cancer Res Treat. 2022. PMID: 36254559 Free PMC article. Review.
-
A comparative study between CT, MRI, and intraoral US for the evaluation of the depth of invasion in early stage (T1/T2) tongue squamous cell carcinoma.Oral Radiol. 2022 Jan;38(1):114-125. doi: 10.1007/s11282-021-00533-7. Epub 2021 May 10. Oral Radiol. 2022. PMID: 33970389 Free PMC article.
-
Electric Bioimpedance Sensing for the Detection of Head and Neck Squamous Cell Carcinoma.Diagnostics (Basel). 2023 Jul 24;13(14):2453. doi: 10.3390/diagnostics13142453. Diagnostics (Basel). 2023. PMID: 37510197 Free PMC article.
-
Image-Guided Intraoperative Assessment of Surgical Margins in Oral Cavity Squamous Cell Cancer: A Diagnostic Test Accuracy Review.Diagnostics (Basel). 2023 May 25;13(11):1846. doi: 10.3390/diagnostics13111846. Diagnostics (Basel). 2023. PMID: 37296701 Free PMC article. Review.
-
Accuracy of magnetic resonance imaging in the assessment of depth of invasion in tongue carcinoma: A systematic review and meta-analysis.Natl J Maxillofac Surg. 2023 Sep-Dec;14(3):341-353. doi: 10.4103/njms.njms_174_22. Epub 2023 Nov 10. Natl J Maxillofac Surg. 2023. PMID: 38273911 Free PMC article. Review.
References
-
- Edge SB, Byrd DR, Compton CC, et al. AJCC cancer staging manual. 7. New York Dordrecht Heidelberg London, Chicago: Springer; 2010.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
