

Dose prediction for repurposing nitazoxanide in SARS-CoV-2 treatment or chemoprophylaxis
- PMID: 33085781
- PMCID: PMC8056737
- DOI: 10.1111/bcp.14619
Dose prediction for repurposing nitazoxanide in SARS-CoV-2 treatment or chemoprophylaxis
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been declared a global pandemic and urgent treatment and prevention strategies are needed. Nitazoxanide, an anthelmintic drug, has been shown to exhibit in vitro activity against SARS-CoV-2. The present study used physiologically based pharmacokinetic (PBPK) modelling to inform optimal doses of nitazoxanide capable of maintaining plasma and lung tizoxanide exposures above the reported SARS-CoV-2 EC90 .
Methods: A whole-body PBPK model was validated against available pharmacokinetic data for healthy individuals receiving single and multiple doses between 500 and 4000 mg with and without food. The validated model was used to predict doses expected to maintain tizoxanide plasma and lung concentrations above the EC90 in >90% of the simulated population. PopDes was used to estimate an optimal sparse sampling strategy for future clinical trials.
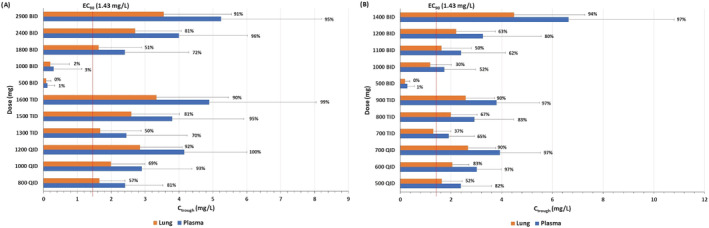
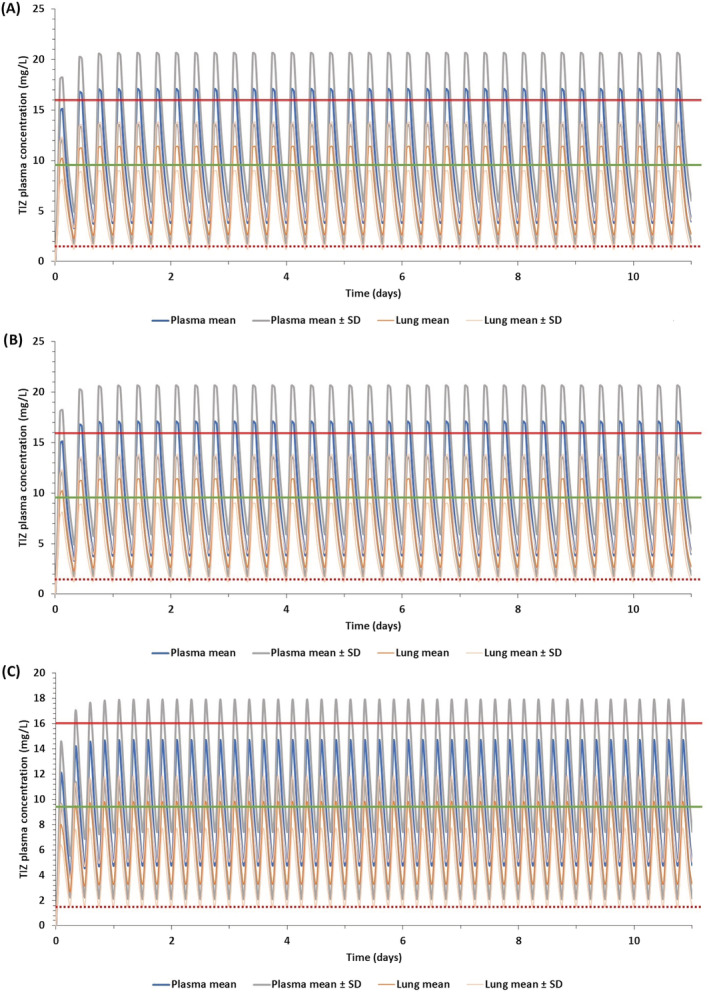
Results: The PBPK model was successfully validated against the reported human pharmacokinetics. The model predicted optimal doses of 1200 mg QID, 1600 mg TID and 2900 mg BID in the fasted state and 700 mg QID, 900 mg TID and 1400 mg BID when given with food. For BID regimens an optimal sparse sampling strategy of 0.25, 1, 3 and 12 hours post dose was estimated.
Conclusion: The PBPK model predicted tizoxanide concentrations within doses of nitazoxanide already given to humans previously. The reported dosing strategies provide a rational basis for design of clinical trials with nitazoxanide for the treatment or prevention of SARS-CoV-2 infection. A concordant higher dose of nitazoxanide is now planned for investigation in the seamless phase I/IIa AGILE trial.
Keywords: COVID-19; SARS-CoV-2; coronavirus; lung; pharmacokinetics.
© 2020 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
A.O. and S.P.R. are Directors of Tandem Nano Ltd. A.O. has received research funding from ViiV, Merck, Janssen and consultancy from Gilead, ViiV and Merck not related to the current paper. P.O.N. is currently engaged in a collaboration with Romark LLC but this interaction did not influence the prioritisation or conclusions in the current manuscript. No other conflicts are declared by the authors.
Figures

Update of
-
Dose prediction for repurposing nitazoxanide in SARS-CoV-2 treatment or chemoprophylaxis.medRxiv [Preprint]. 2020 May 6:2020.05.01.20087130. doi: 10.1101/2020.05.01.20087130. medRxiv. 2020. Update in: Br J Clin Pharmacol. 2021 Apr;87(4):2078-2088. doi: 10.1111/bcp.14619. PMID: 32511548 Free PMC article. Updated. Preprint.
References
-
- Johns Hopkins University of Medicine . Coronavirus Resource Center. 2020 [cited 2020 17/04/2020]; Available from: https://coronavirus.jhu.edu/map.html
-
- Gns HS, Gr S, Murahari M, Krishnamurthy M. An update on drug repurposing: re‐written saga of the drug's fate. Biomed Pharmacother. 2019;110:700‐716. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
