

Multimorbidity among incident Finnish systemic lupus erythematosus patients during 2000-2017
- PMID: 33086917
- PMCID: PMC7768886
- DOI: 10.1177/0961203320967102
Multimorbidity among incident Finnish systemic lupus erythematosus patients during 2000-2017
Abstract
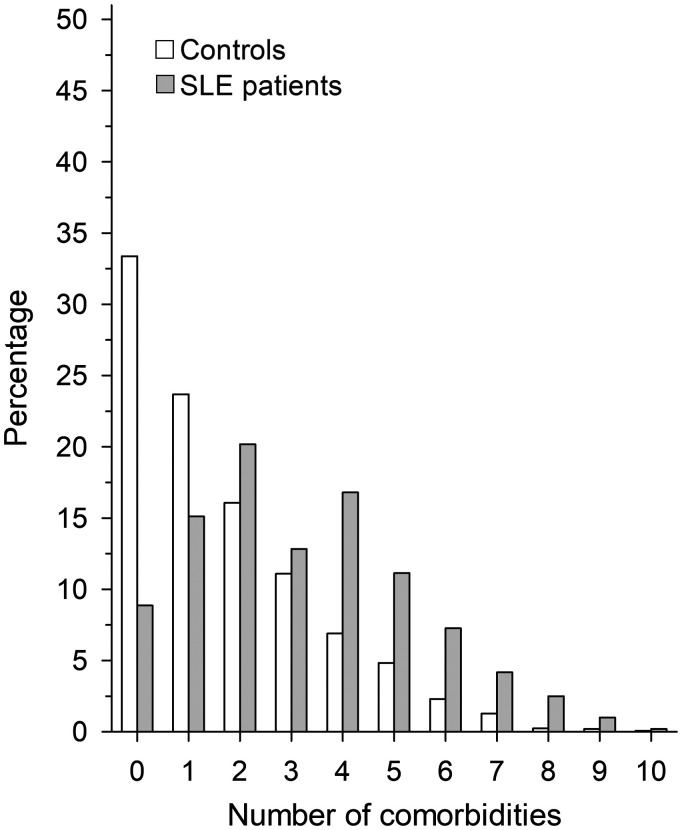
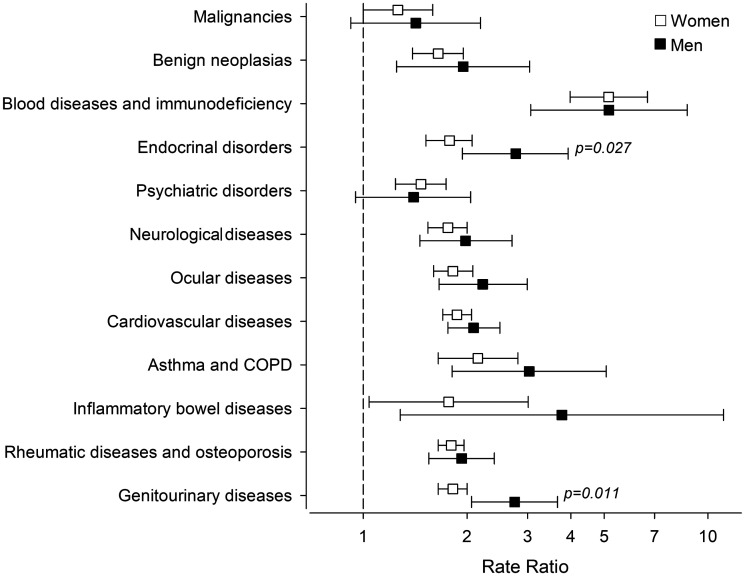
The objective of the study was to examine the risk of other morbidities among patients with systemic lupus erythematosus (SLE). A total of 1006 adult new-onset SLE patients were identified during 1.1.2000- 31.12.2014 from the register of Social Insurance Institution. For each case three general population controls matched according to age, sex and place of residence at the index day were sampled from the population register. Both groups were followed up from the index date until the end of 2017 or until death. The national register on specialized care was explored to gather broadly their 12 organ-specific morbidities, which were found among 91.2% of SLE patients and 66.7% of comparators. The rate ratio (RR) was elevated in almost all disease groups. Musculoskeletal, cardiovascular and genitourinary conditions were the most common comorbidities with RRs of 1.82 (1.68 to 1.97), 1.91 (1.76 to 2.08) and 1.91 (1.73 to 2.09), respectively. Men with SLE had a significantly higher risk for diseases of the genitourinary system and endocrine, nutritional and metabolic diseases compared to women with SLE. The risk of concurrent morbidities is essential to note in the care of SLE patients.
Keywords: Systemic lupus erythematosus; cardiovascular disease; comorbidity; gender; morbidity.
Conflict of interest statement
Figures
References
-
- Cervera R, Abarca-Costalago M, Abramovicz D, et al. ; European Working Party on Systemic Lupus Erythematosus. Systemic lupus erythematosus in Europe at the change of the millennium: lessons from the “Euro-Lupus project”. Autoimmun Rev 2006; 5: 180–186. - PubMed
-
- Sarkissian A, Sivaraman V, Bout-Tabaku S, et al. Bone turnover markers in relation to vitamin D status and disease activity in adults with systemic lupus erythematosus. Lupus 2019; 28: 156–162. - PubMed
-
- Huang X, Magder LS, Petri M. Predictors of incident depression in systemic lupus erythematosus. J Rheumatol 2014; 41: 1823–1833. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
