

COVID-19: What Iodine Maps From Perfusion CT can reveal-A Prospective Cohort Study
- PMID: 33087155
- PMCID: PMC7576979
- DOI: 10.1186/s13054-020-03333-3
COVID-19: What Iodine Maps From Perfusion CT can reveal-A Prospective Cohort Study
Abstract
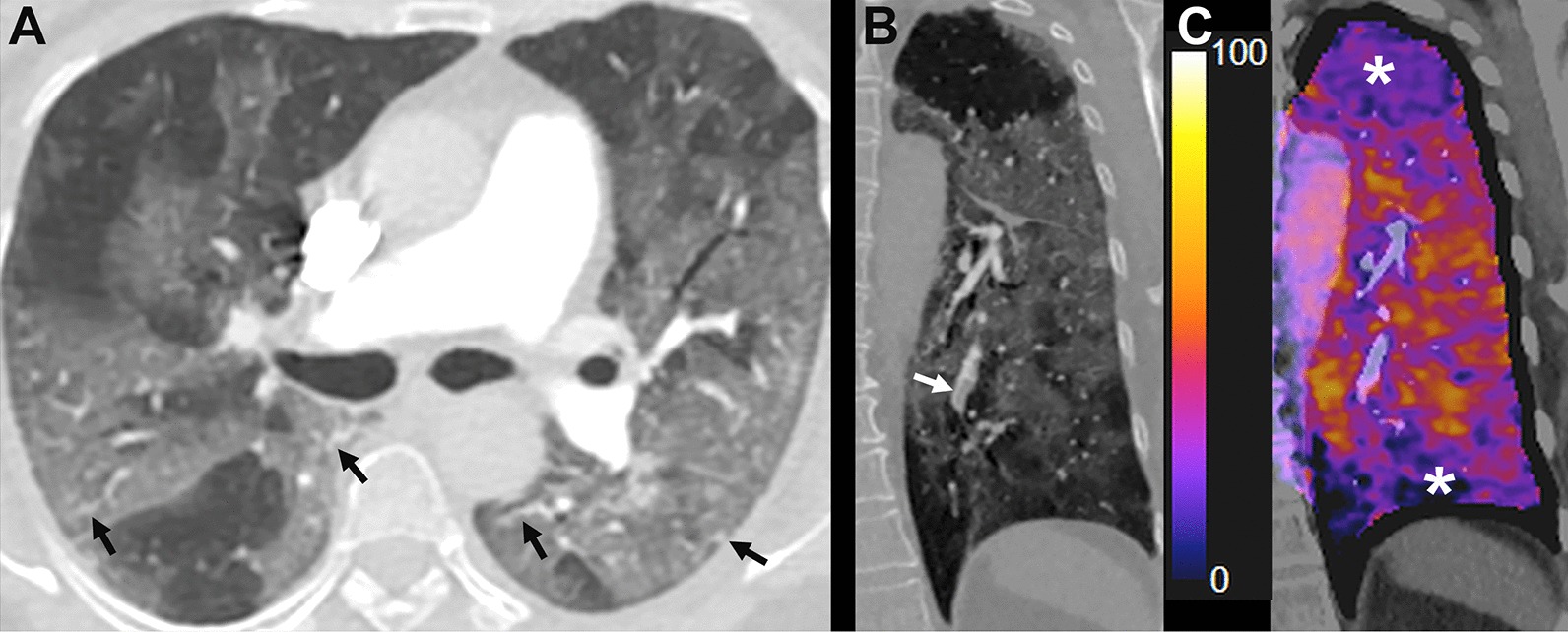
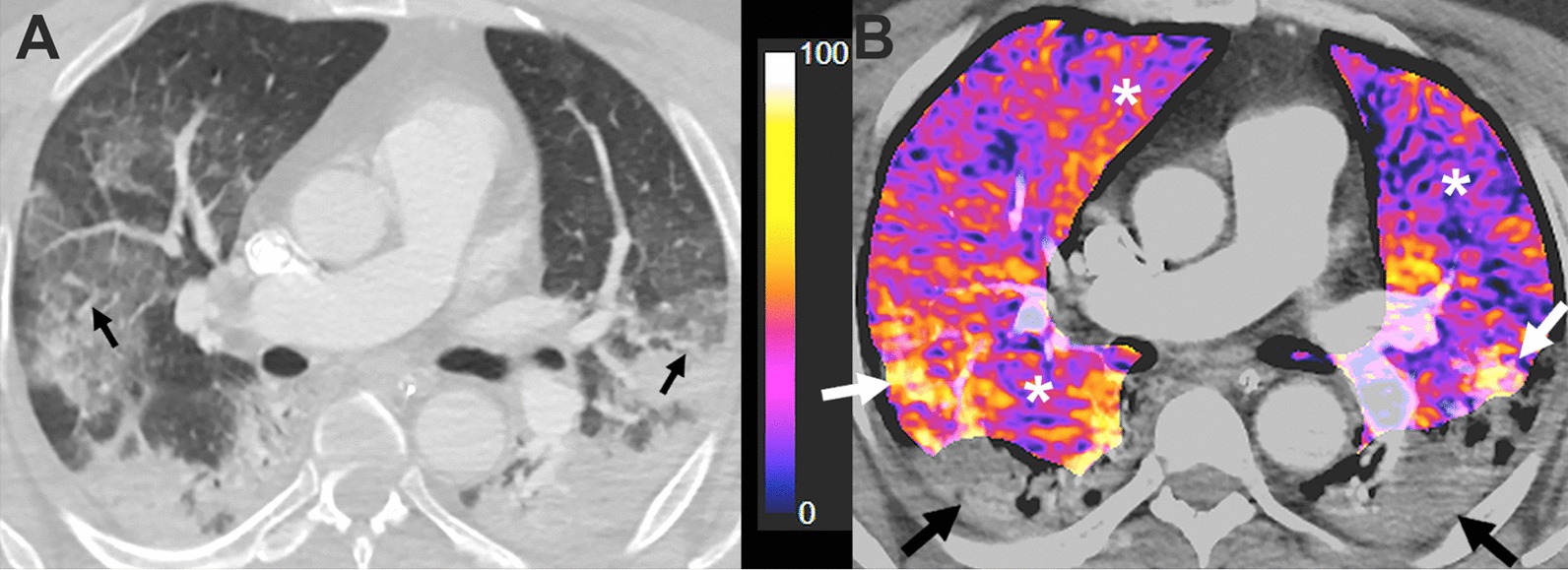
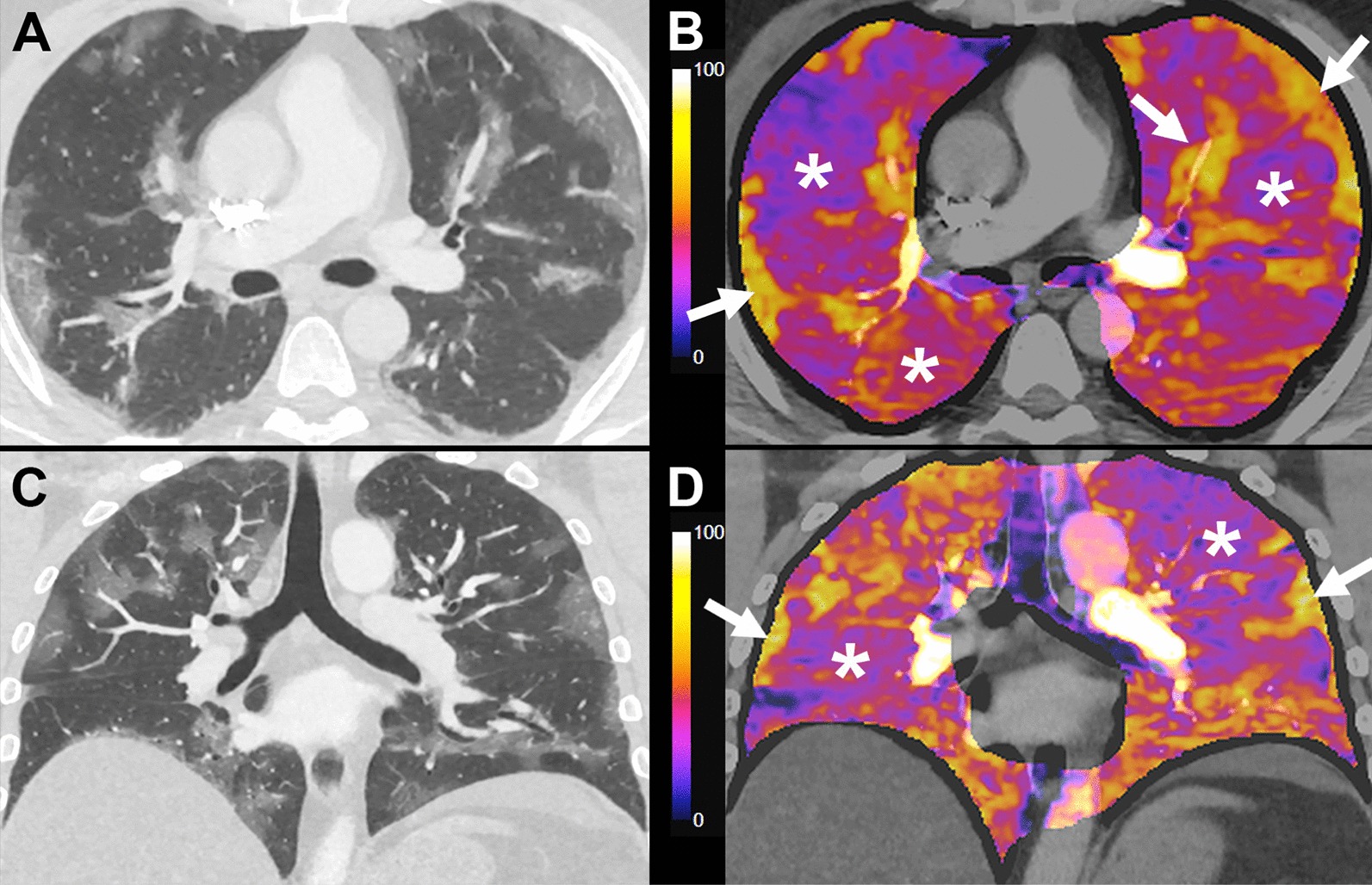
Background: Subtraction CT angiography (sCTA) is a technique used to evaluate pulmonary perfusion based on iodine distribution maps. The aim of this study is to assess lung perfusion changes with sCTA seen in patients with COVID-19 pneumonia and correlate them with clinical outcomes.
Material and methods: A prospective cohort study was carried out with 45 RT-PCR-confirmed COVID-19 patients that required hospitalization at three different hospitals, between April and May 2020. In all cases, a basic clinical and demographic profile was obtained. Lung perfusion was assessed using sCTA. Evaluated imaging features included: Pattern predominance of injured lung parenchyma in both lungs (ground-glass opacities, consolidation and mixed pattern) and anatomical extension; predominant type of perfusion abnormality (increased perfusion or hypoperfusion), perfusion abnormality distribution (focal or diffuse), extension of perfusion abnormalities (mild, moderate and severe involvement); presence of vascular dilatation and vascular tortuosity. All participants were followed-up until hospital discharge searching for the development of any of the study endpoints. These endpoints included intensive-care unit (ICU) admission, initiation of invasive mechanical ventilation (IMV) and death.
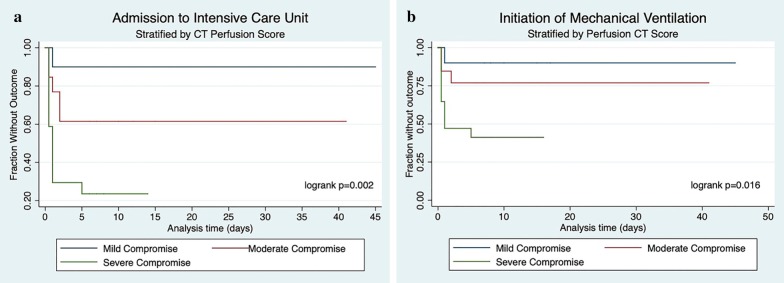
Results: Forty-one patients (55.2 ± 16.5 years, 22 men) with RT-PCR-confirmed SARS-CoV-2 infection and an interpretable iodine map were included. Patients with perfusion anomalies on sCTA in morphologically normal lung parenchyma showed lower Pa/Fi values (294 ± 111.3 vs. 397 ± 37.7, p = 0.035), and higher D-dimer levels (1156 ± 1018 vs. 378 ± 60.2, p < 0.01). The main common patterns seen in lung CT scans were ground-glass opacities, mixed pattern with predominant ground-glass opacities and mixed pattern with predominant consolidation in 56.1%, 24.4% and 19.5% respectively. Perfusion abnormalities were common (36 patients, 87.8%), mainly hypoperfusion in areas of apparently healthy lung. Patients with severe hypoperfusion in areas of apparently healthy lung parenchyma had an increased probability of being admitted to ICU and to initiate IMV (HR of 11.9 (95% CI 1.55-91.9) and HR 7.8 (95% CI 1.05-61.1), respectively).
Conclusion: Perfusion abnormalities evidenced in iodine maps obtained by sCTA are associated with increased admission to ICU and initiation of IMV in COVID-19 patients.
Keywords: Angiotensin II; Angiotensin converting enzyme 2; COVID-19; Computed tomography angiography; Coronavirus; Vasoconstriction; Vasoplegia; Ventilation-perfusion ratio.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.html. Accessed 22 July 2020.
-
- Oudkerk M, Büller HR, Kuijpers D, van Es N, Oudkerk SF, McLoud TC, Gommers D, van Dissel J, Ten Cate H, van Beek EJ. Diagnosis, prevention, and treatment of thromboembolic complications in COVID-19: report of the National Institute for Public Health of the Netherlands. Radiology. 2020 doi: 10.1148/radiol.2020201629. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
