

Cognitive phenotypes 1 month after ICU discharge in mechanically ventilated patients: a prospective observational cohort study
- PMID: 33087171
- PMCID: PMC7579874
- DOI: 10.1186/s13054-020-03334-2
Cognitive phenotypes 1 month after ICU discharge in mechanically ventilated patients: a prospective observational cohort study
Abstract
Background: ICU patients undergoing invasive mechanical ventilation experience cognitive decline associated with their critical illness and its management. The early detection of different cognitive phenotypes might reveal the involvement of diverse pathophysiological mechanisms and help to clarify the role of the precipitating and predisposing factors. Our main objective is to identify cognitive phenotypes in critically ill survivors 1 month after ICU discharge using an unsupervised machine learning method, and to contrast them with the classical approach of cognitive impairment assessment. For descriptive purposes, precipitating and predisposing factors for cognitive impairment were explored.
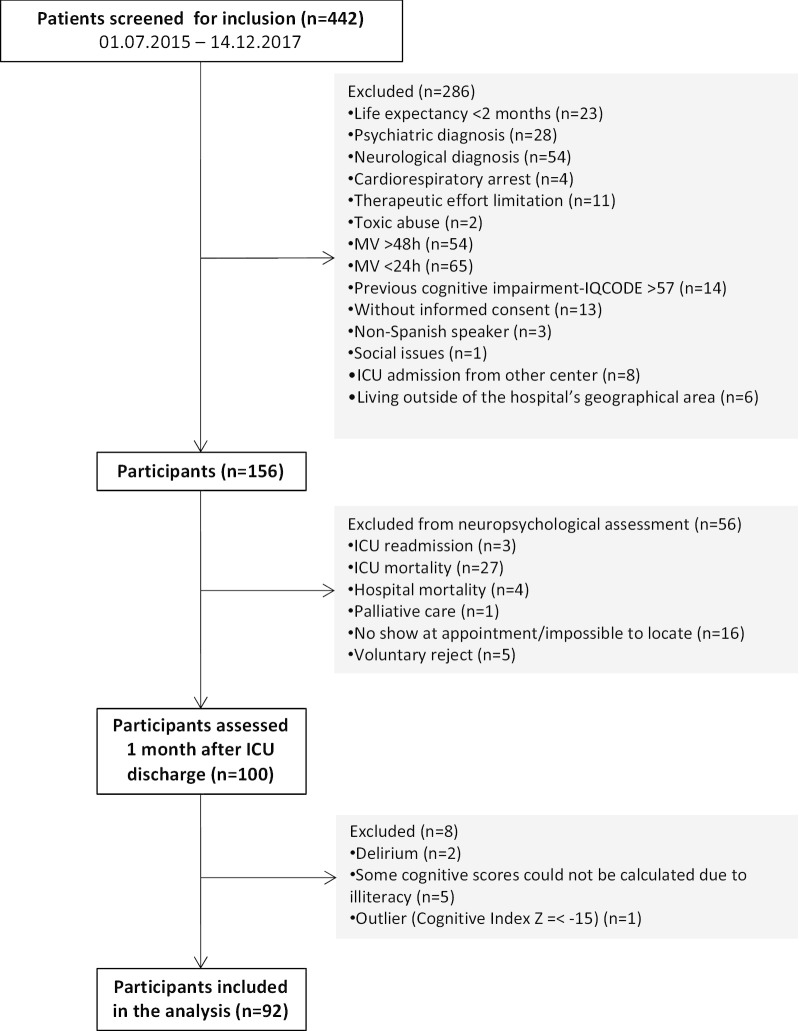
Methods: A total of 156 mechanically ventilated critically ill patients from two medical/surgical ICUs were prospectively studied. Patients with previous cognitive impairment, neurological or psychiatric diagnosis were excluded. Clinical variables were registered during ICU stay, and 100 patients were cognitively assessed 1 month after ICU discharge. The unsupervised machine learning K-means clustering algorithm was applied to detect cognitive phenotypes. Exploratory analyses were used to study precipitating and predisposing factors for cognitive impairment.
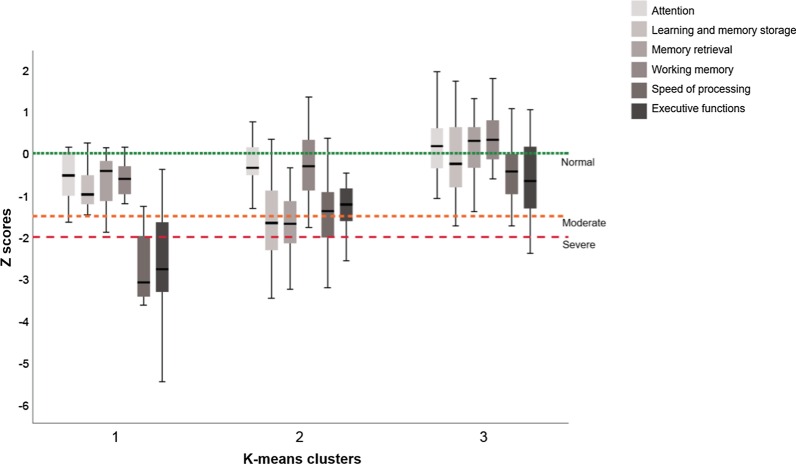
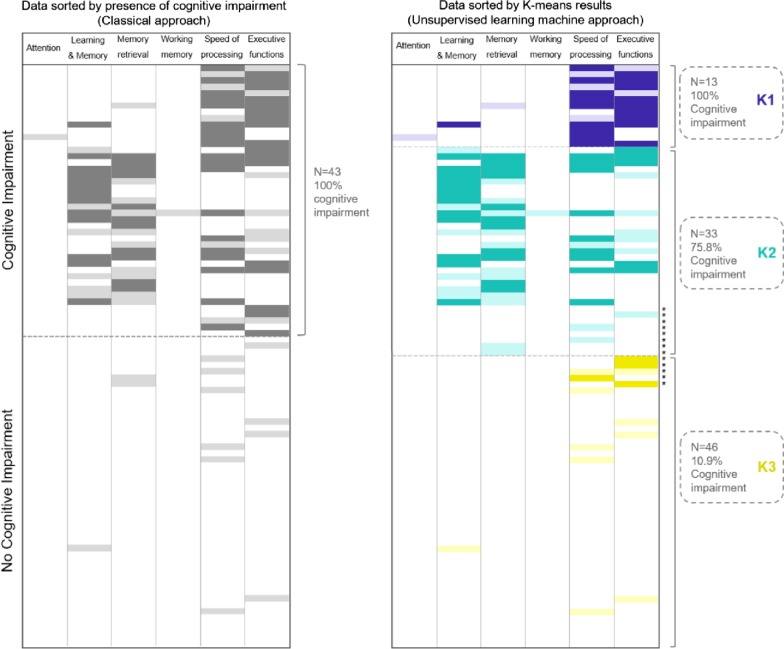
Results: K-means testing identified three clusters (K) of patients with different cognitive phenotypes: K1 (n = 13), severe cognitive impairment in speed of processing (92%) and executive function (85%); K2 (n = 33), moderate-to-severe deficits in learning-memory (55%), memory retrieval (67%), speed of processing (36.4%) and executive function (33.3%); and K3 (n = 46), normal cognitive profile in 89% of patients. Using the classical approach, moderate-to-severe cognitive decline was recorded in 47% of patients, while the K-means method accurately classified 85.9%. The descriptive analysis showed significant differences in days (p = 0.016) and doses (p = 0.039) with opioid treatment in K1 vs. K2 and K3. In K2, there were more women, patients were older and had more comorbidities (p = 0.001) than in K1 or K3. Cognitive reserve was significantly (p = 0.001) higher in K3 than in K1 or K2.
Conclusion: One month after ICU discharge, three groups of patients with different cognitive phenotypes were identified through an unsupervised machine learning method. This novel approach improved the classical classification of cognitive impairment in ICU survivors. In the exploratory analysis, gender, age and the level of cognitive reserve emerged as relevant predisposing factors for cognitive impairment in ICU patients.
Trial registration: ClinicalTrials.gov Identifier:NCT02390024; March 17,2015.
Keywords: Cognition in ICU survivors; Critical illness; Neuropsychological profiles; Post-intensive care syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
