

Altered Gemcitabine and Nab-paclitaxel Scheduling Improves Therapeutic Efficacy Compared with Standard Concurrent Treatment in Preclinical Models of Pancreatic Cancer
- PMID: 33087331
- PMCID: PMC7855515
- DOI: 10.1158/1078-0432.CCR-20-1422
Altered Gemcitabine and Nab-paclitaxel Scheduling Improves Therapeutic Efficacy Compared with Standard Concurrent Treatment in Preclinical Models of Pancreatic Cancer
Abstract
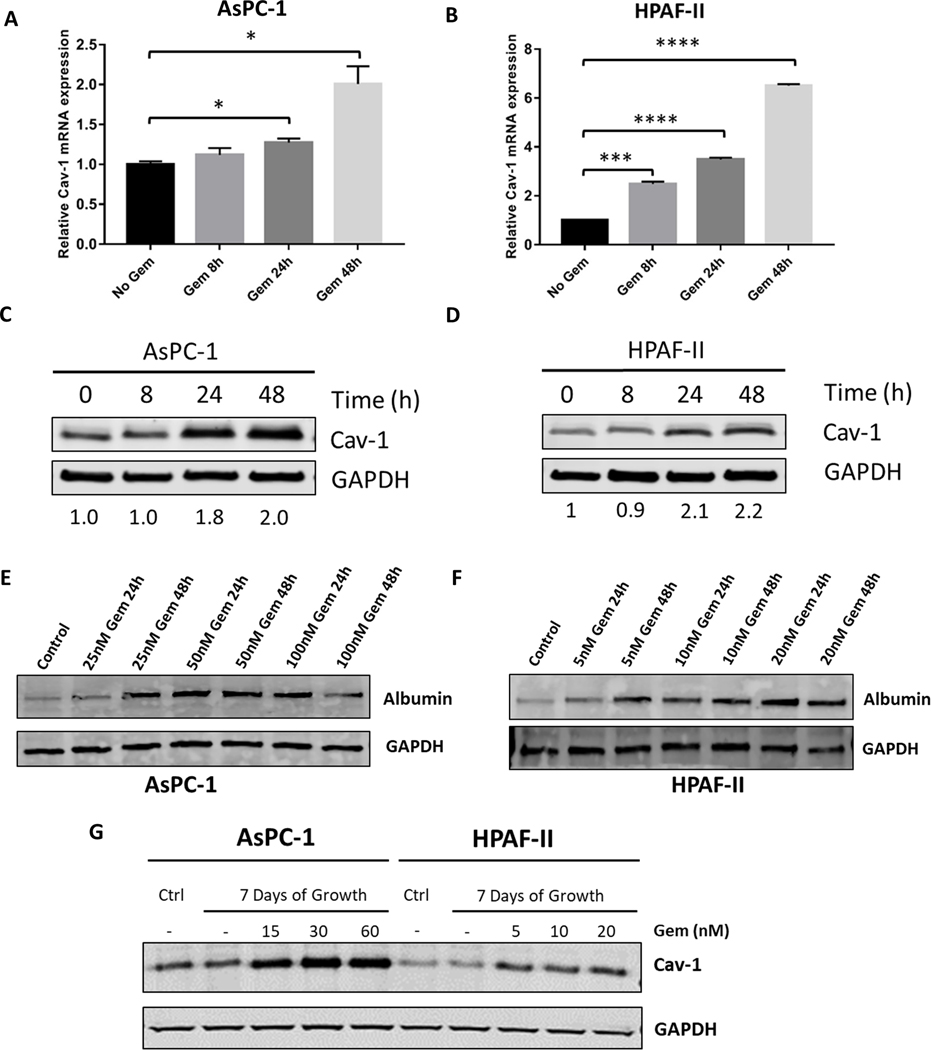
Purpose: Concurrent gemcitabine and nab-paclitaxel treatment is one of the preferred chemotherapy regimens for metastatic and locally advanced pancreatic ductal adenocarcinoma (PDAC). Previous studies demonstrate that caveolin-1 (Cav-1) expression is critical for nab-paclitaxel uptake into tumors and correlates with response. Gemcitabine increases nab-paclitaxel uptake by increasing Cav-1 expression. Thus, we hypothesized that pretreatment with gemcitabine would further enhance the sensitivity of PDAC to nab-paclitaxel by increasing Cav-1 expression and nab-paclitaxel uptake.
Experimental design: We investigated the sensitivity of different gemcitabine and nab-paclitaxel treatment regimens in a panel of PDAC cell lines and orthotopic xenograft models. The sensitivity of different treatment regimens was compared with the standard concurrent treatment.
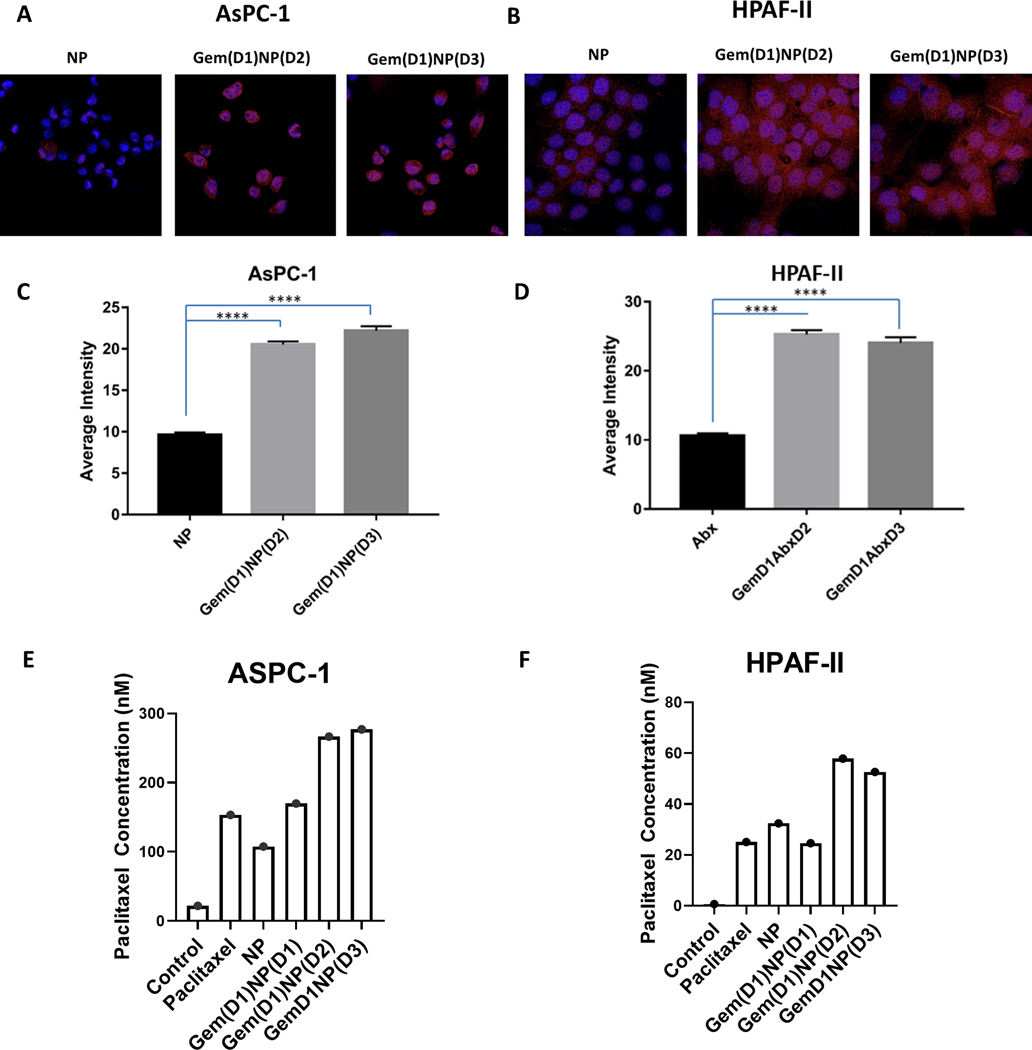
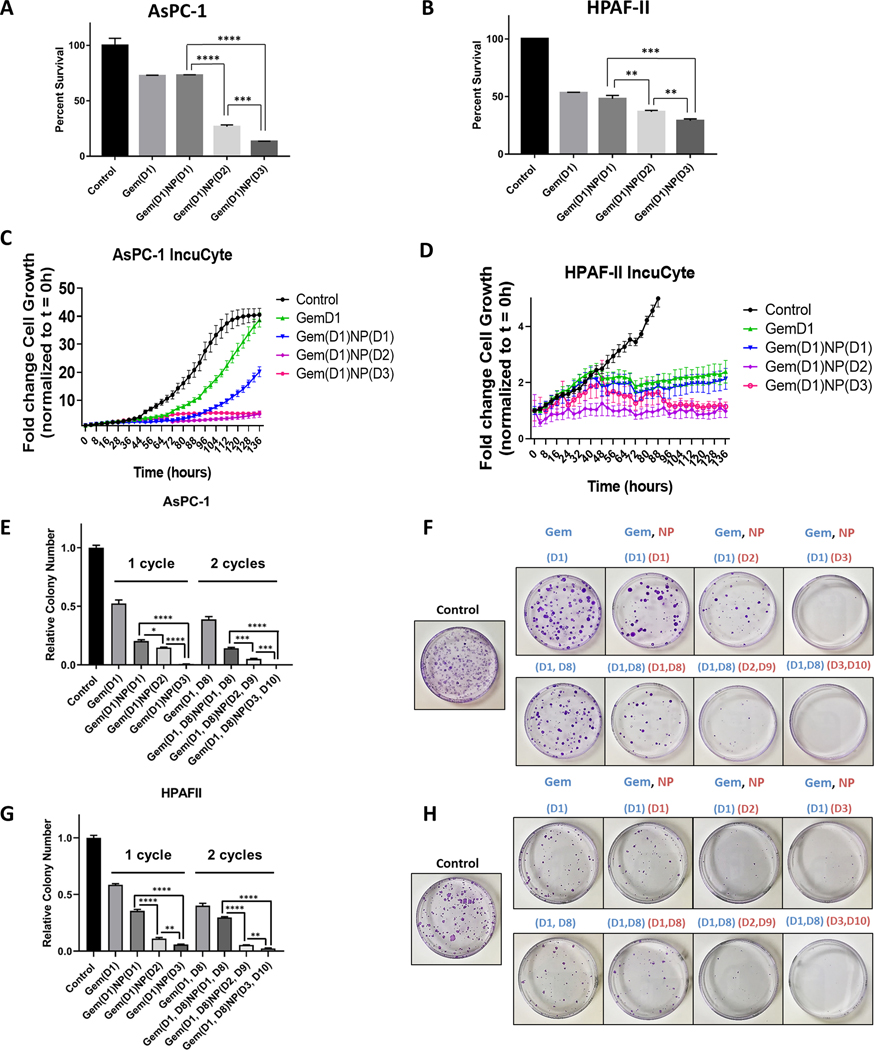
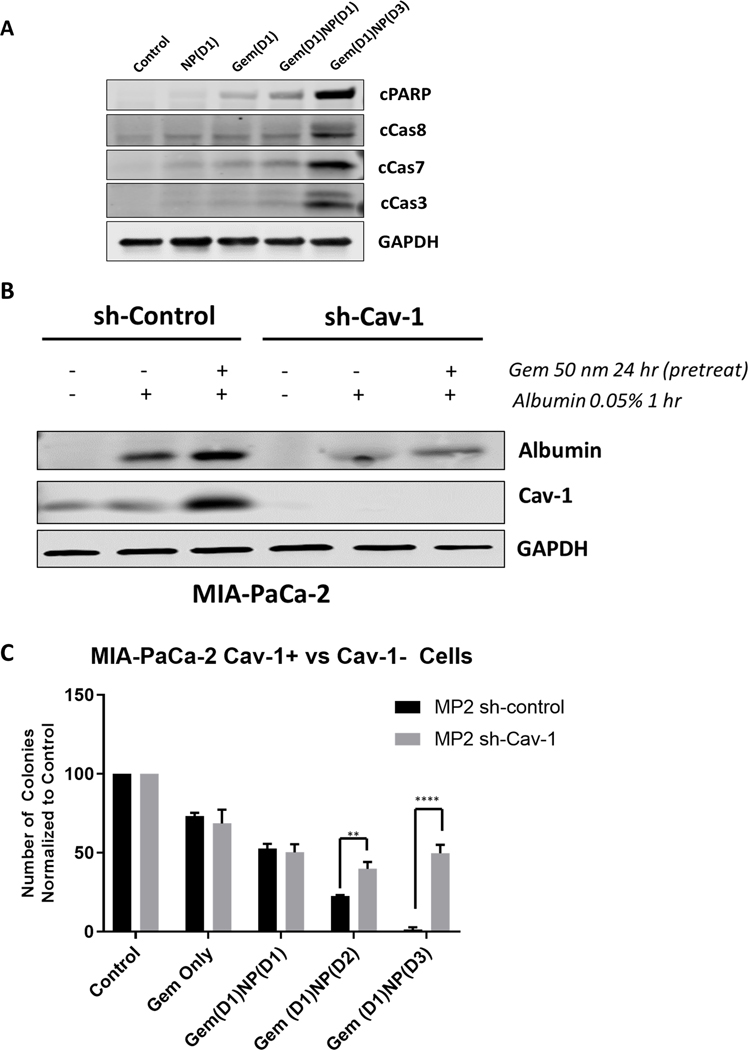
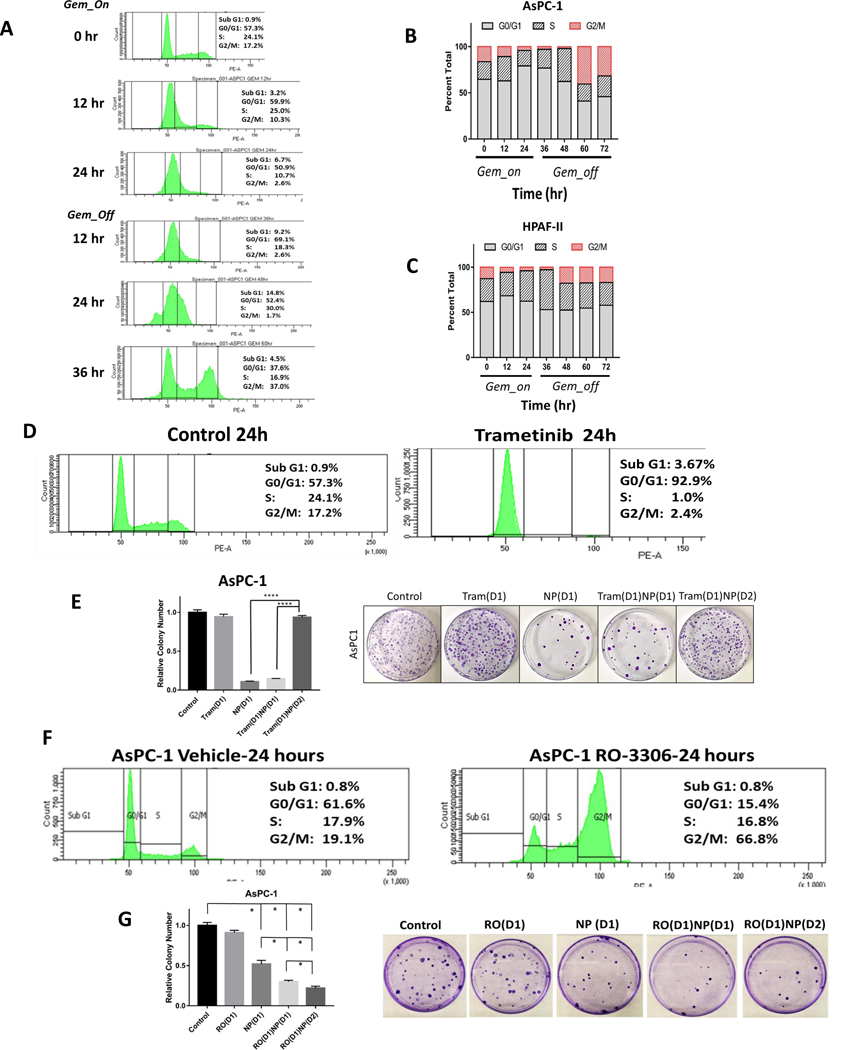
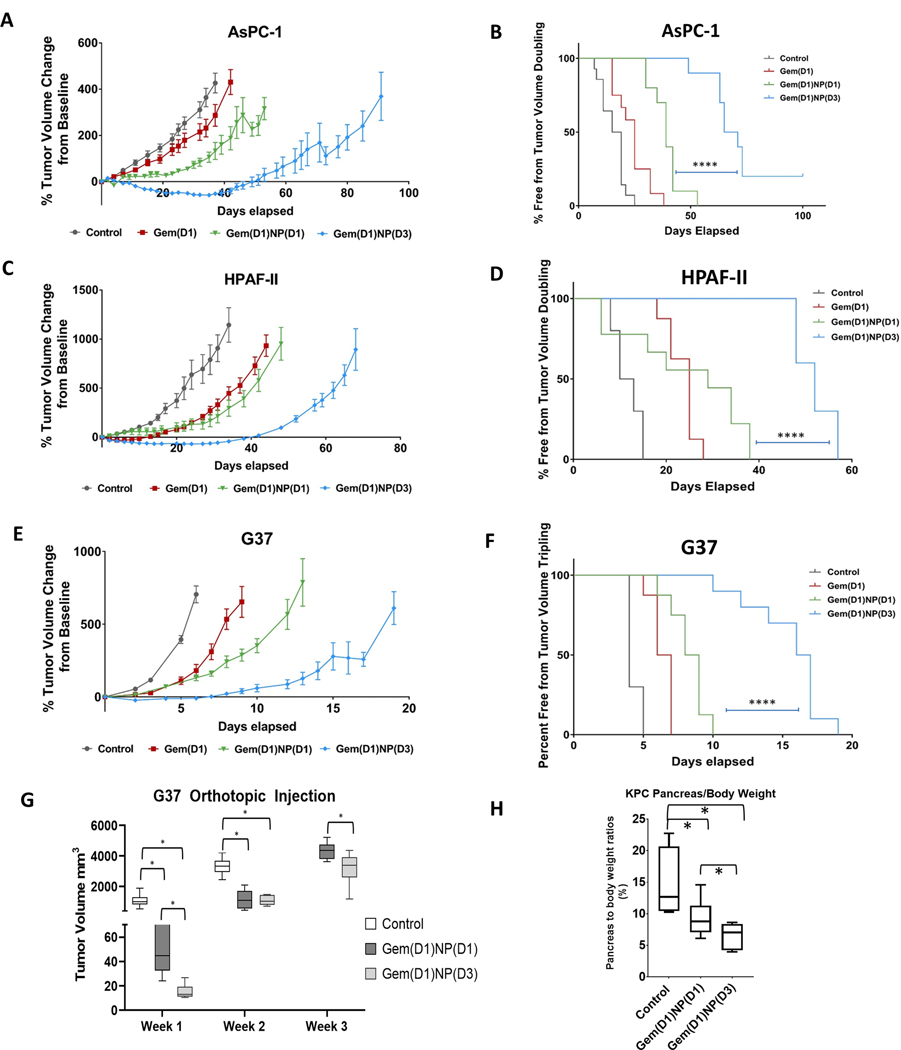
Results: Pretreatment with gemcitabine before nab-paclitaxel increased Cav-1 and albumin uptake and significantly decreased proliferation and clonogenicity compared with concurrent treatment, which correlated with increased levels of apoptosis. Cav-1 silencing reduced the uptake of albumin, and therapeutic advantage was observed when cells were pretreated with gemcitabine prior to nab-paclitaxel. In addition, we observed that pretreatment with gemcitabine resulted in partial synchronization of cells in the G2-M-phase at the time of nab-paclitaxel treatment, providing another mechanism for the benefit of altered scheduling. In heterotopic and orthotopic xenograft models, the altered schedule of gemcitabine prior to nab-paclitaxel significantly delayed tumor growth compared with concurrent delivery without added toxicity.
Conclusions: Pretreatment with gemcitabine significantly increased nab-paclitaxel uptake and correlated with an increased treatment efficacy and survival benefit in preclinical models, compared with standard concurrent treatment. These results justify preclinical and clinical testing of this altered scheduling combination.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, and Jemal A. Cancer statistics, 2020. CA: A Cancer Journal for Clinicians. 2020;70(1):7–30. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, and Matrisian LM. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Research. 2014;74(11):2913–21. - PubMed
-
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15(6):2403–13. - PubMed
-
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. Jama. 2013;310(14):1473–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
