

Electronic DNA Analysis of CSF Cell-free Tumor DNA to Quantify Multi-gene Molecular Response in Pediatric High-grade Glioma
- PMID: 33087334
- PMCID: PMC7710567
- DOI: 10.1158/1078-0432.CCR-20-2066
Electronic DNA Analysis of CSF Cell-free Tumor DNA to Quantify Multi-gene Molecular Response in Pediatric High-grade Glioma
Abstract
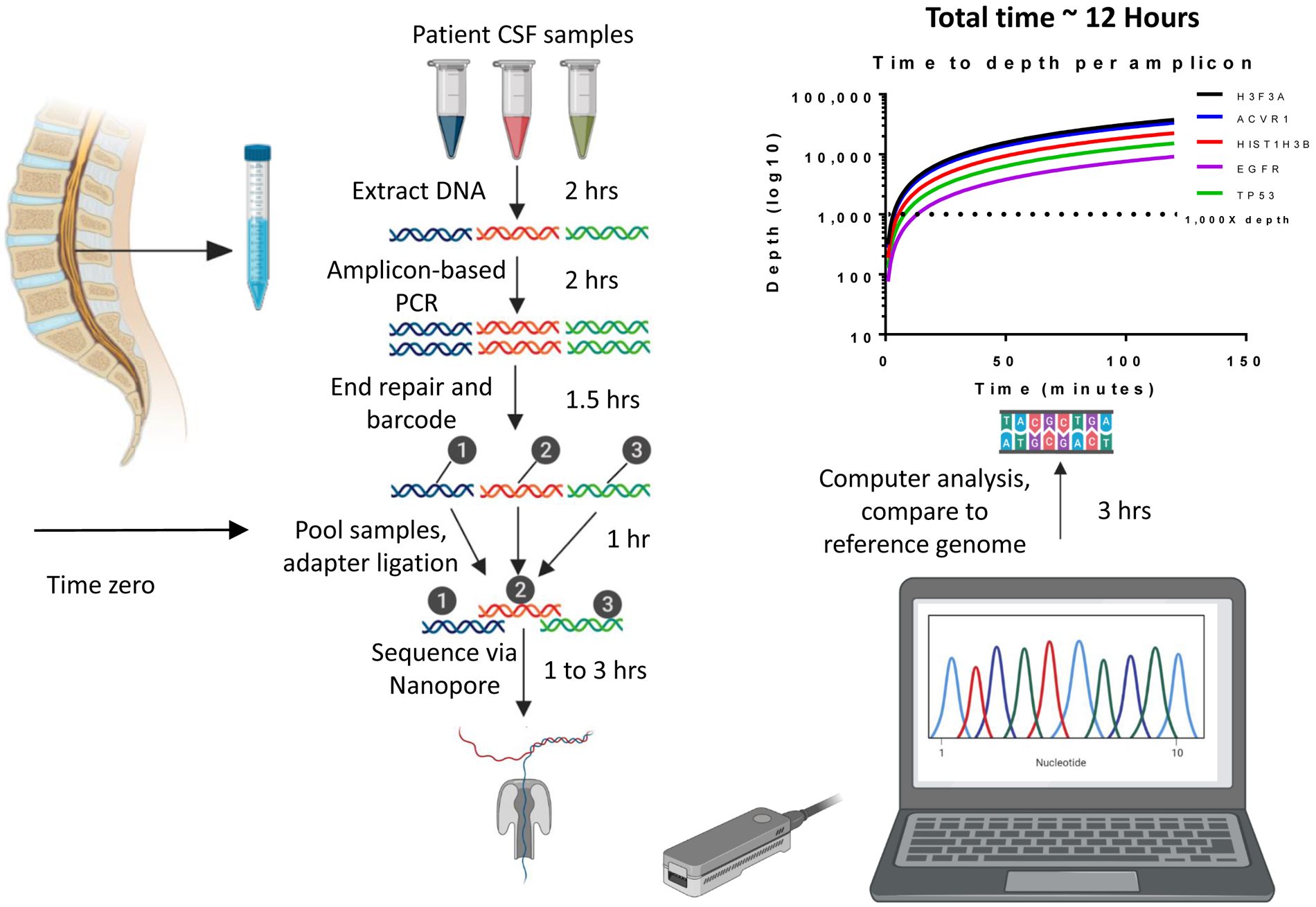
Purpose: Pediatric high-grade glioma (pHGG) diagnosis portends poor prognosis and therapeutic monitoring remains difficult. Tumors release cell-free tumor DNA (cf-tDNA) into cerebrospinal fluid (CSF), allowing for potential detection of tumor-associated mutations by CSF sampling. We hypothesized that direct, electronic analysis of cf-tDNA with a handheld platform (Oxford Nanopore MinION) could quantify patient-specific CSF cf-tDNA variant allele fraction (VAF) with improved speed and limit of detection compared with established methods.
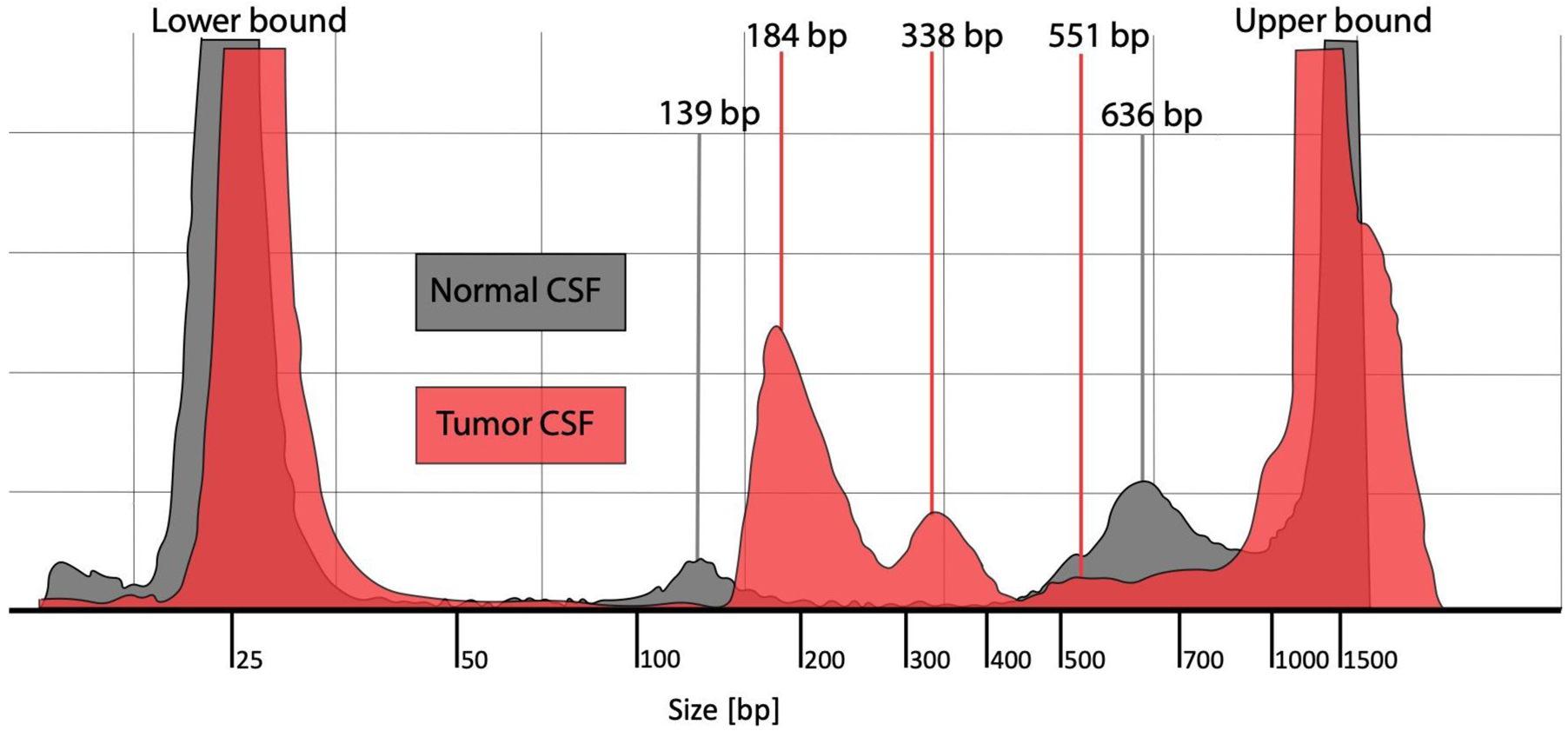
Experimental design: We performed ultra-short fragment (100-200 bp) PCR amplification of cf-tDNA for clinically actionable alterations in CSF and tumor samples from patients with pHGG (n = 12) alongside nontumor CSF (n = 6). PCR products underwent rapid amplicon-based sequencing by Oxford Nanopore Technology (Nanopore) with quantification of VAF. Additional comparison to next-generation sequencing (NGS) and droplet digital PCR (ddPCR) was performed.
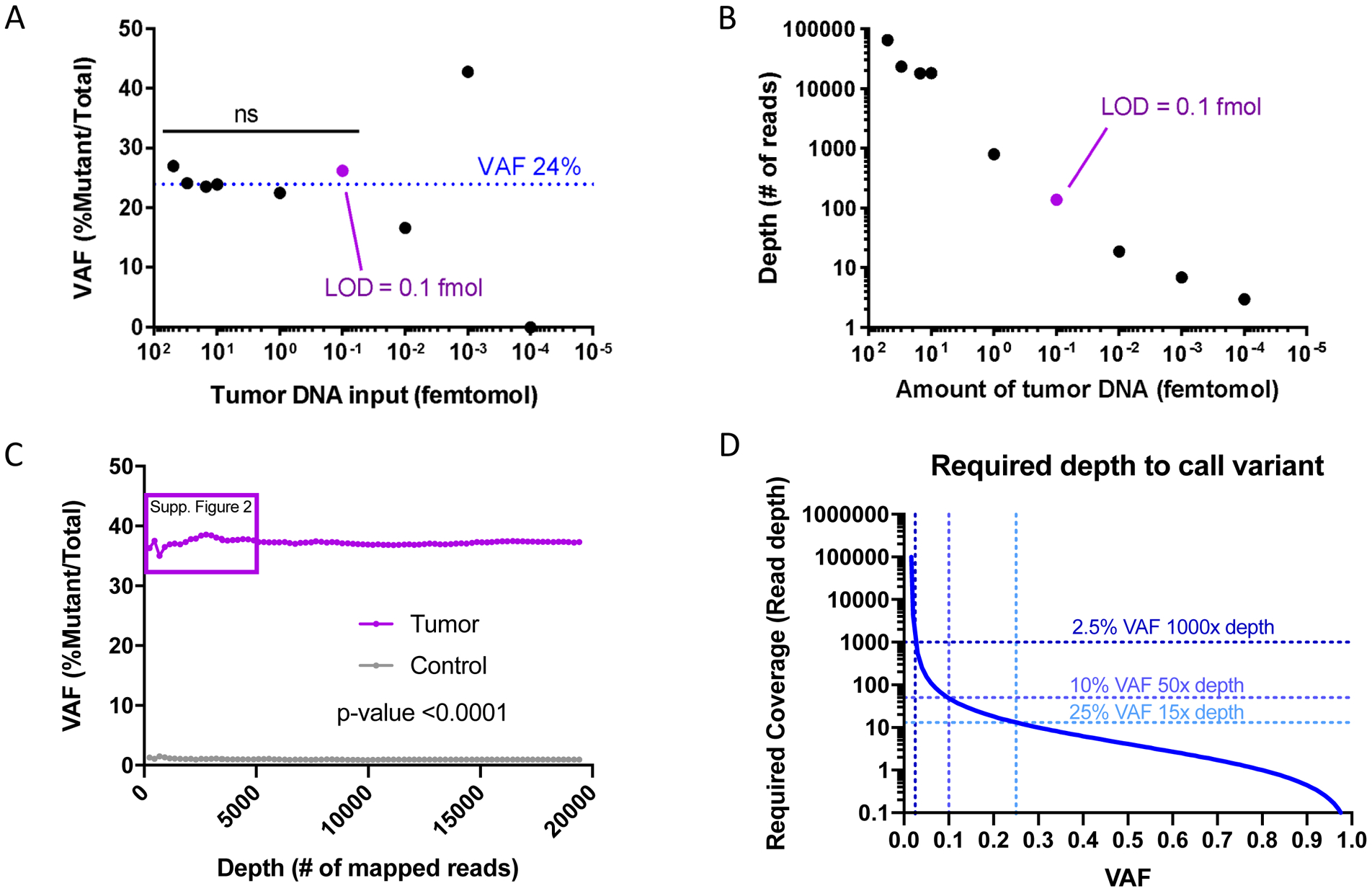
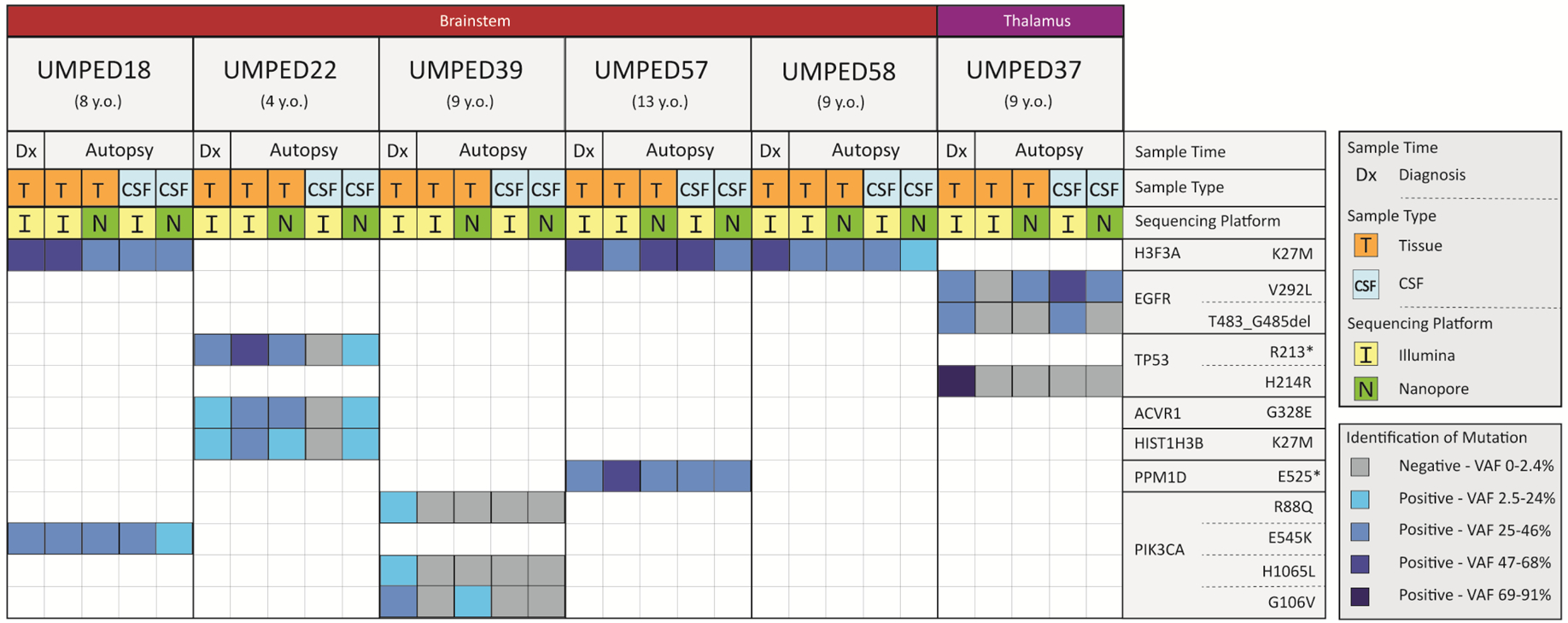
Results: Nanopore demonstrated 85% sensitivity and 100% specificity in CSF samples (n = 127 replicates) with 0.1 femtomole DNA limit of detection and 12-hour results, all of which compared favorably with NGS. Multiplexed analysis provided concurrent analysis of H3.3A (H3F3A) and H3C2 (HIST1H3B) mutations in a nonbiopsied patient and results were confirmed by ddPCR. Serial CSF cf-tDNA sequencing by Nanopore demonstrated correlation of radiological response on a clinical trial, with one patient showing dramatic multi-gene molecular response that predicted long-term clinical response.
Conclusions: Nanopore sequencing of ultra-short pHGG CSF cf-tDNA fragments is feasible, efficient, and sensitive with low-input samples thus overcoming many of the barriers restricting wider use of CSF cf-tDNA diagnosis and monitoring in this patient population.
©2020 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest:
None of the authors have potential conflicts of interest.
Figures

References
-
- Hoffman LM, Veldhuijzen van Zanten SEM, Colditz N, Baugh J, Chaney B, Hoffmann M, et al. Clinical, Radiologic, Pathologic, and Molecular Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma (DIPG): A Collaborative Report From the International and European Society for Pediatric Oncology DIPG Registries. J Clin Oncol 2018;36(19):1963–72 doi 10.1200/JCO.2017.75.9308. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
