

Impact of Intraoperative 3-Tesla MRI on Endonasal Endoscopic Pituitary Adenoma Resection and a Proposed New Scoring System for Predicting the Utility of Intraoperative MRI
- PMID: 33087635
- PMCID: PMC7788269
- DOI: 10.2176/nmc.oa.2020-0060
Impact of Intraoperative 3-Tesla MRI on Endonasal Endoscopic Pituitary Adenoma Resection and a Proposed New Scoring System for Predicting the Utility of Intraoperative MRI
Abstract
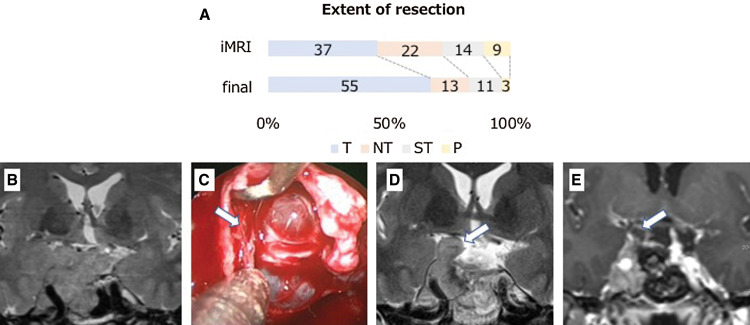
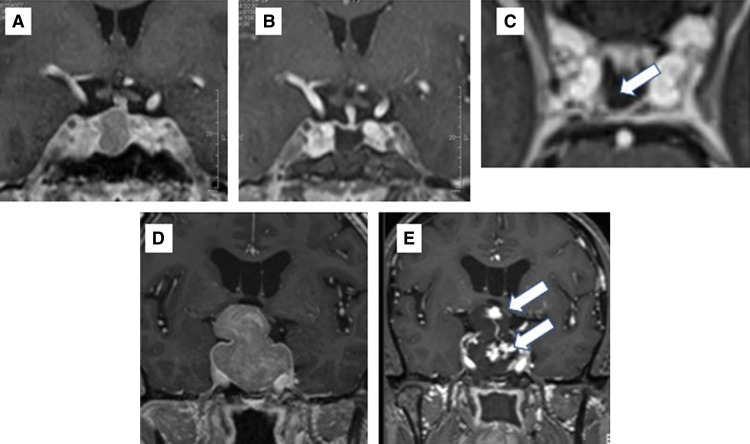
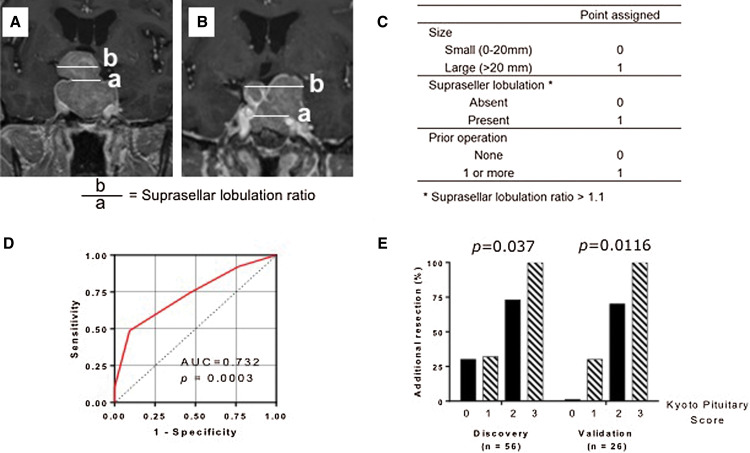
The aim of this study was to evaluate the impact of 3-Tesla intraoperative high-field magnetic resonance imaging (3T-iMRI) for pituitary adenoma resection, and to propose a new scoring system for predicting the utility of 3T-iMRI. This retrospective study evaluated 82 patients with pituitary adenoma who underwent purely endoscopic endonasal resection with 3T-iMRI between 2015 and 2019. 3T-iMRI revealed unexpected residual tumor in 39 cases (47.6%), which led to further resection and contributed to upgrading of the resection level in 28 cases (34.1%), which led to gross total resection rates (GTRs) of 67.1% and near total resection of 15.9%. To construct a new scoring system, patients were divided into a discovery cohort (56 patients) and a validation cohort (26 patients). Three variables for the scoring system were selected according to a univariate analysis of the discovery cohort: the size of the tumor (>20 mm: 1 point), the presence of suprasellar tumor lobulation (1 point) and the history of previous operations (1 point). The risk of additional resection after iMRI was well stratified by this scoring system (range 0-3; p = 0.0037 for trend). Robustness of the system was confirmed in the validation cohort (0 points, 0%; 1 point, 30.8%; 2 points, 70.0%; 3 points, 100%; p = 0.0116 for trend). These results indicate that 3T-iMRI optimized the extent of resection, even with the use of an endoscope, and that the proposed scoring system is useful for predicting whether 3T-iMRI is likely to be of value for a particular patient.
Keywords: Knosp grade; intraoperative MRI; pituitary score; pituitary surgery; transsphenoidal surgery.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
-
- Kassam AB, Prevedello DM, Carrau RL, et al. : Endoscopic endonasal skull base surgery: analysis of complications in the authors’ initial 800 patients. J Neurosurgery 114: 1544–1568, 2011 - PubMed
-
- de Divitiis E, Laws ER, Giani U, Iuliano SL, de Divitiis O, Apuzzo ML: The current status of endoscopy in transsphenoidal surgery: an international survey. World Neurosurg 83: 447–454, 2015 - PubMed
-
- Soneru CP, Riley CA, Hoffman K, Tabaee A, Schwartz TH: Intra-operative MRI vs endoscopy in achieving gross total resection of pituitary adenomas: a systematic review. Acta Neurochir (Wien) 161: 1683–1698, 2019 - PubMed
-
- Fahlbusch R, Golby A, Prada F, Zada G: Utility of intraoperative imaging. Neurosurg Focus 40: 1610, 2016 - PubMed