Estrogen hormone replacement therapy in incidental intracranial meningioma: a growth-rate analysis
- PMID: 33087798
- PMCID: PMC7578640
- DOI: 10.1038/s41598-020-74344-x
Estrogen hormone replacement therapy in incidental intracranial meningioma: a growth-rate analysis
Abstract
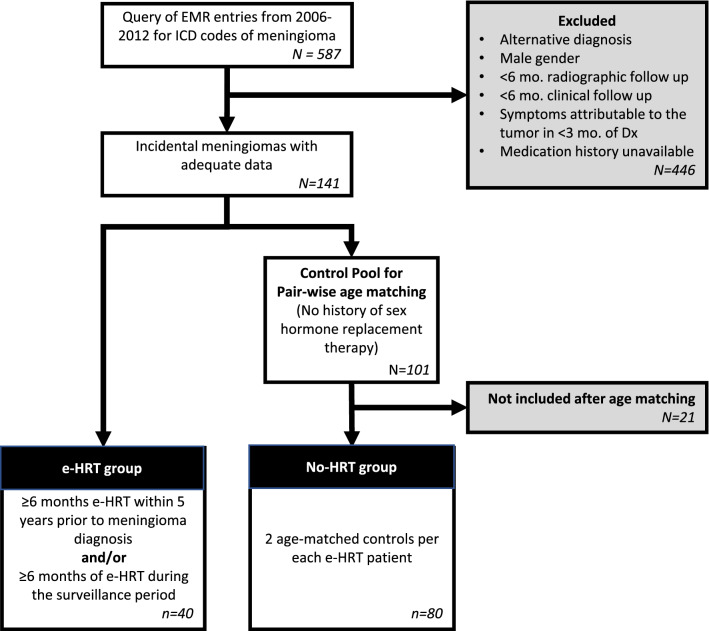
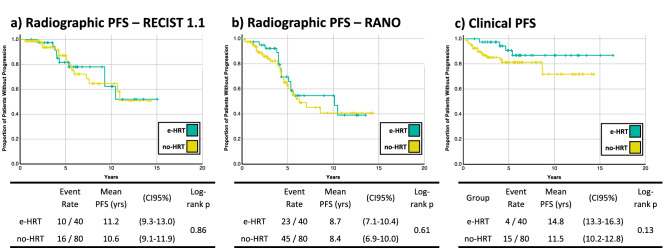
Incidental meningiomas (IMs) are the most common intracranial neoplasms, especially in perimenopausal women. There is ongoing debate on whether their incidence is increased by hormone replacement therapy. Meningiomas often express estrogen receptors, which were linked to higher proliferative activity according to some reports. Consequently, there is a theoretical risk of estrogen-based HRT (e-HRT) leading to an increase in tumor growth and thus altering the natural history of IMs. However, clinical data is lacking to support this notion. To identify differences in the natural history of IM after e-HRT exposure. We queried the NorthShore Meningioma Database for patients with ≥ 6 months of e-HRT. They were compared with age-matched IM controls. Forty patients were included in the e-HRT group (mean age 62.1 ± 12.0 years; mean duration of HRT 5.3 ± 4.5 years) and 80 in the no-HRT group (mean age 62.2 ± 12 years). Radiographic appearance was similar between groups. The average 2D tumor diameter was 35% lower in the e-HRT group (p = 0.02), with an absolute growth-rate of half of the no-HRT group (p = 0.02). Radiographic and clinical progression-free survival were 1.2 years and 3.3 years longer in the e-HRT group, respectively. These preliminary results suggest that e-HRT may be safe in incidental meningiomas.
Conflict of interest statement
The authors declare no competing interests.
Figures