

Total Sacrectomy for the Treatment of Advanced Pelvic Chondrosarcoma
- PMID: 33088124
- PMCID: PMC7534767
- DOI: 10.1007/s13193-019-01009-1
Total Sacrectomy for the Treatment of Advanced Pelvic Chondrosarcoma
Abstract
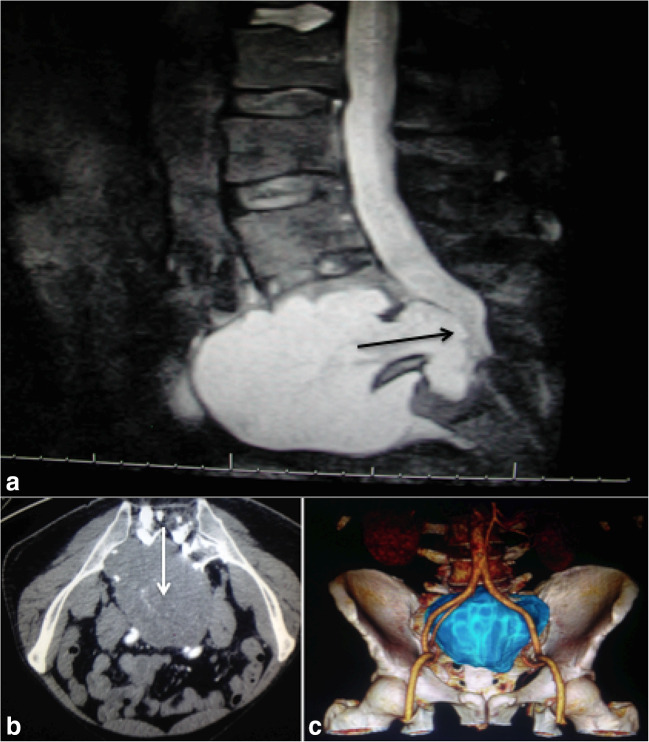
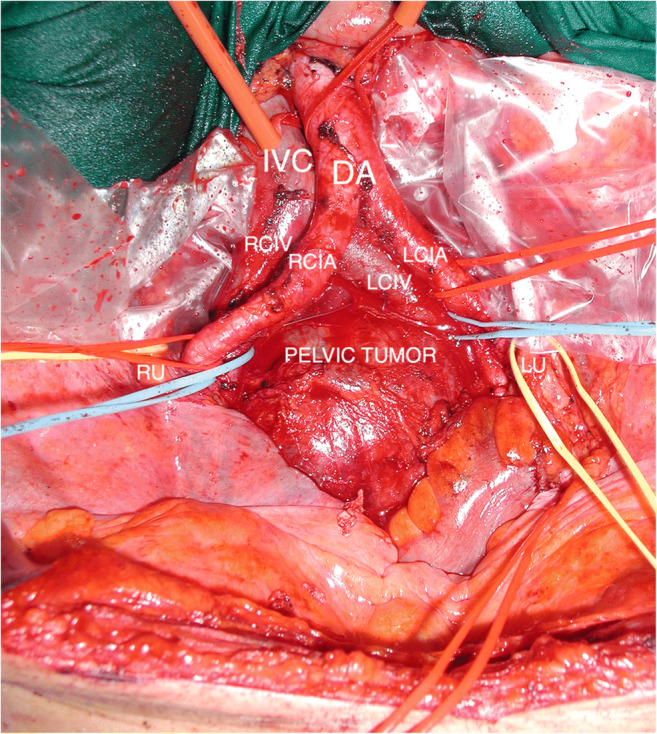
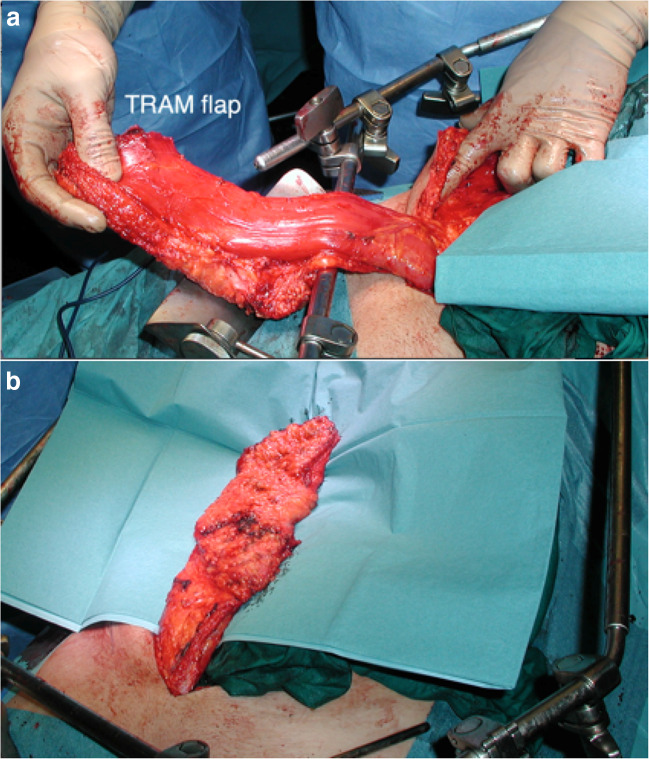
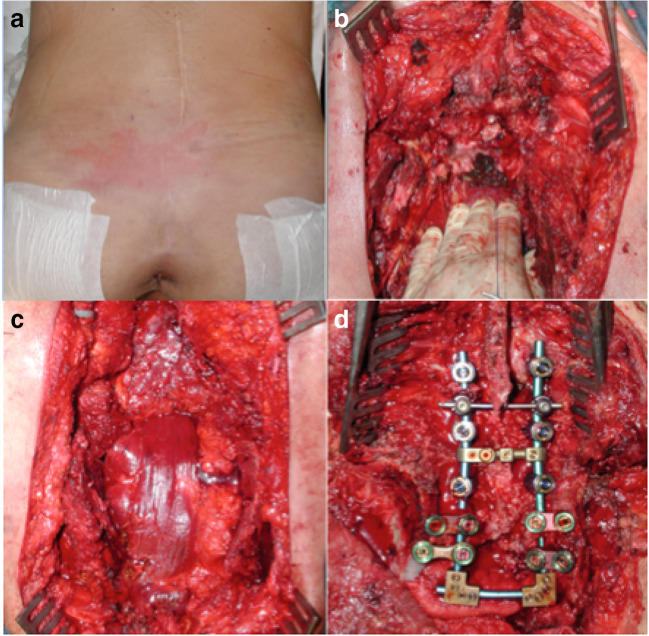
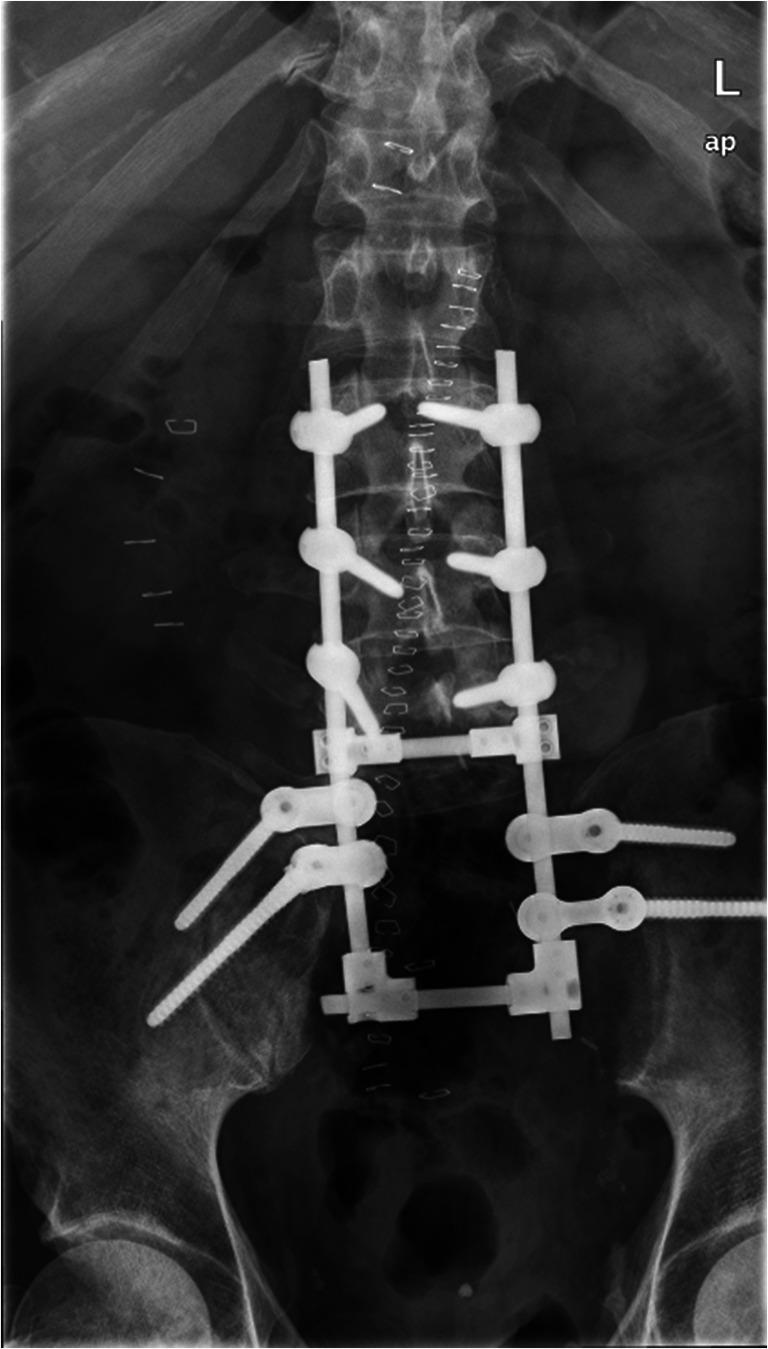
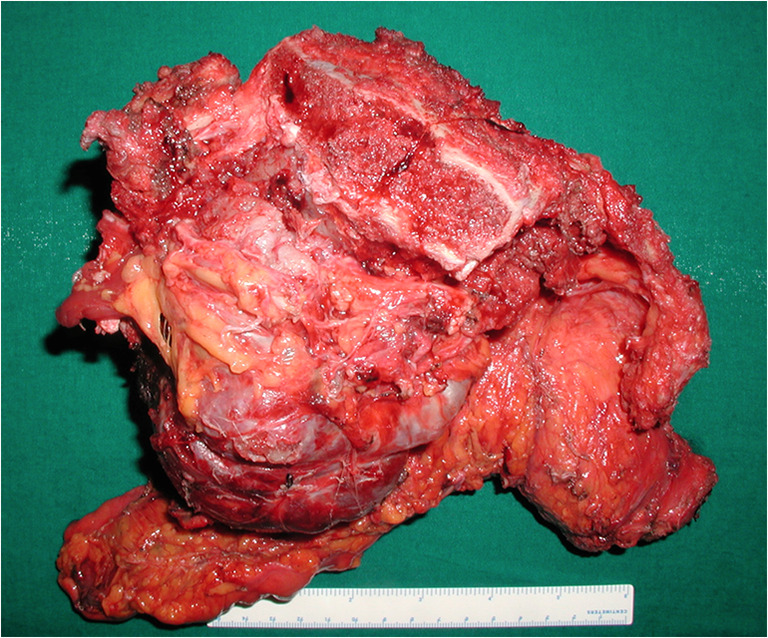
Primary tumors of sacrum are rare. The most common malignant tumors are metastasis, and only 6% of all malignant tumors arise from the sacrum. Chondrosarcoma is the third most common primary bone malignancy following myeloma and osteosarcoma. Surgery is usually the most important therapeutic modality; the wide en bloc excision remains the treatment of choice. These technically demanding procedures require a multidisciplinary expert team (neurosurgery, surgical and orthopedic oncology, colorectal surgery, and plastic surgery) involvement. We present in this article a case of a 52-year-old man who presented less infrequent symptoms, and the diagnosis was made in a very advanced stage. The wide surgical excision of the mass was performed by two different anterior and posterior approaches in one stage. The free surgical margins were difficult to achieve because it presented a voluminous tumor with invasion of the rectum, bone, and sacral plexus, but the age, low histological grade, and extensive experience in extreme pelvic surgery of our multidisciplinary team allowed approaching the patient with debulking surgery en bloc, successfully. Total hospital stay was 20 days. The patient was discharged without any complications. At the 6-months' follow-up, the patient showed no local recurrence.
Keywords: Chondrosarcoma; Multidisciplinary; Sacrectomy.
© Indian Association of Surgical Oncology 2019.
Figures
References
-
- Mavrogenis AF, Pavlos P, Georgia K, Papagelopoulos Panayiotis J. Tumours of the sacrum. Orthop. 2009;32:5–5. - PubMed
-
- Hogendoorn PCW, Bovee JM, Nielsen GP. Chondrosarcoma (grades I-III), including primary and secondary variants and periosteal chondrosarcoma. In: CDM F, Bridge JA, PCW H, Mertens F, editors. World Health Organization classification of tumours of soft tissue and bone. 4. Lyon: IARC; 2013. p. 264.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials