

Emergence of T cell immunosenescence in diabetic chronic kidney disease
- PMID: 33088331
- PMCID: PMC7574244
- DOI: 10.1186/s12979-020-00200-1
Emergence of T cell immunosenescence in diabetic chronic kidney disease
Abstract
Background: Type 2 diabetes is an important challenge given the worldwide epidemic and is the most important cause of end-stage renal disease (ESRD) in developed countries. It is known that patients with ESRD and advanced renal failure suffer from immunosenescence and premature T cell aging, but whether such changes develop in patients with less severe chronic kidney disease (CKD) is unclear.
Method: 523 adult patients with type 2 diabetes were recruited for this study. Demographic data and clinical information were obtained from medical chart review. Immunosenescence, or aging of the immune system was assessed by staining freshly-obtained peripheral blood with immunophenotyping panels and analyzing cells using multicolor flow cytometry.
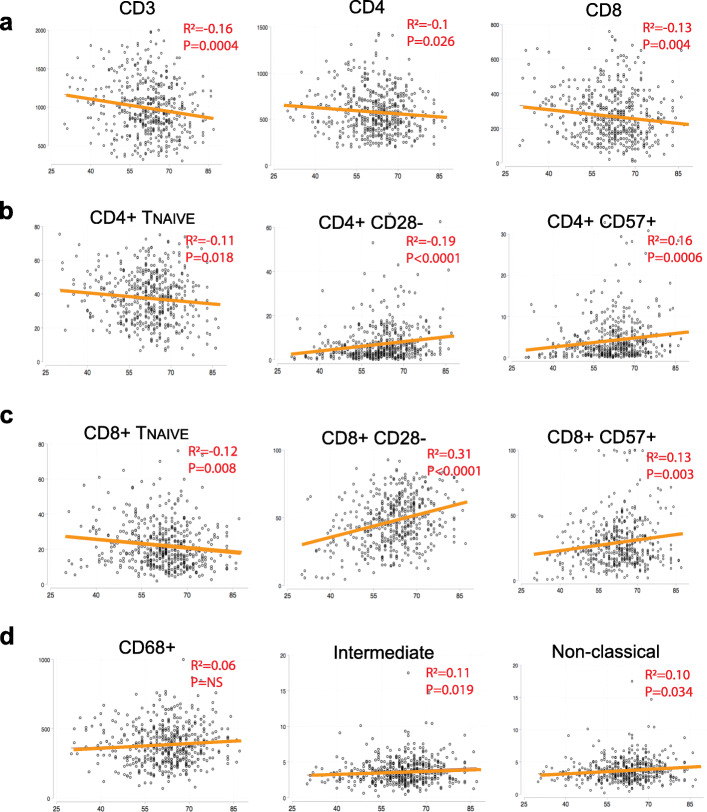
Result: Consistent with previously observed in the general population, both T and monocyte immunosenescence in diabetic patients positively correlate with age. When compared to diabetic patients with preserved renal function (estimated glomerular filtration rate > 60 ml/min), patients with impaired renal function exhibit a significant decrease of total CD3+ and CD4+ T cells, but not CD8+ T cell and monocyte numbers. Immunosenescence was observed in patients with CKD stage 3 and in patients with more severe renal failure, especially of CD8+ T cells. However, immunosenescence was not associated with level of proteinuria level or glucose control. In age, sex and glucose level-adjusted regression models, stage 3 CKD patients exhibited significantly elevated percentages of CD28-, CD127-, and CD57+ cells among CD8+ T cells when compared to patients with preserved renal function. In contrast, no change was detected in monocyte subpopulations as renal function declined. In addition, higher body mass index (BMI) is associated with enhanced immunosenescence irrespective of CKD status.
Conclusion: The extent of immunosenescence is not significantly associated with proteinuria or glucose control in type 2 diabetic patients. T cells, especially the CD8+ subsets, exhibit aggravated characteristics of immunosenescence during renal function decline as early as stage 3 CKD. In addition, inflammation increases since stage 3 CKD and higher BMI drives the accumulation of CD8+CD57+ T cells. Our study indicates that therapeutic approaches such as weight loss may be used to prevent the emergence of immunosenescence in diabetes before stage 3 CKD.
Keywords: BMI; CKD; Diabetes; Immunosenescence; T cell.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsNon-declared. The authors declare that the research was conducted in the absence of any commercial or financial relationships that serves as a potential conflict of interest. The results presented in this paper have not been published previously in whole or part, except in abstract format.
Figures
Similar articles
-
Shifts in subsets of CD8+ T-cells as evidence of immunosenescence in patients with cancers affecting the lungs: an observational case-control study.BMC Cancer. 2015 Dec 28;15:1016. doi: 10.1186/s12885-015-2013-3. BMC Cancer. 2015. PMID: 26711627 Free PMC article.
-
T-Lymphocyte Subsets Alteration, Infection and Renal Outcome in Advanced Chronic Kidney Disease.Front Med (Lausanne). 2021 Sep 9;8:742419. doi: 10.3389/fmed.2021.742419. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34568395 Free PMC article.
-
A comprehensive characterization of aggravated aging-related changes in T lymphocytes and monocytes in end-stage renal disease: the iESRD study.Immun Ageing. 2018 Nov 8;15:27. doi: 10.1186/s12979-018-0131-x. eCollection 2018. Immun Ageing. 2018. PMID: 30455721 Free PMC article.
-
The immune system in extreme longevity.Exp Gerontol. 2008 Feb;43(2):61-5. doi: 10.1016/j.exger.2007.06.008. Epub 2007 Jul 4. Exp Gerontol. 2008. PMID: 17870272 Review.
-
Immune dysfunction in patients with end stage kidney disease; Immunosenescence - Review.Rom J Intern Med. 2024 Mar 23;62(1):12-19. doi: 10.2478/rjim-2023-0030. Print 2024 Mar 1. Rom J Intern Med. 2024. PMID: 37991332 Review.
Cited by
-
T-Cell Senescence in Human Metabolic Diseases.Diabetes Metab J. 2024 Sep;48(5):864-881. doi: 10.4093/dmj.2024.0140. Epub 2024 Aug 28. Diabetes Metab J. 2024. PMID: 39192822 Free PMC article. Review.
-
Inflammation and gut dysbiosis as drivers of CKD-MBD.Nat Rev Nephrol. 2023 Oct;19(10):646-657. doi: 10.1038/s41581-023-00736-7. Epub 2023 Jul 24. Nat Rev Nephrol. 2023. PMID: 37488276 Review.
-
Identification of Anoikis-Related Genes in Chronic Kidney Disease Based on Bioinformatics Analysis Combined with Experimental Validation.J Inflamm Res. 2025 Jan 21;18:973-994. doi: 10.2147/JIR.S498820. eCollection 2025. J Inflamm Res. 2025. PMID: 39867944 Free PMC article.
-
Epigenetic quantification of immunosenescent CD8+ TEMRA cells in human blood.Aging Cell. 2022 May;21(5):e13607. doi: 10.1111/acel.13607. Epub 2022 Apr 9. Aging Cell. 2022. PMID: 35397197 Free PMC article.
-
Identification of crucial genes and possible molecular pathways associated with active vitamin D intervention in diabetic kidney disease.Heliyon. 2024 Sep 25;10(19):e38334. doi: 10.1016/j.heliyon.2024.e38334. eCollection 2024 Oct 15. Heliyon. 2024. PMID: 39398062 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
