

The rate of intraspinal problems and clinical evaluation of scoliosis: A cross-sectional, descriptive study
- PMID: 33089089
- PMCID: PMC7557620
- DOI: 10.5606/tftrd.2020.4527
The rate of intraspinal problems and clinical evaluation of scoliosis: A cross-sectional, descriptive study
Abstract
Objectives: This study aims to define the chronological, angular, and topographic classes in presumed idiopathic scoliosis and to investigate the frequency of generalized joint hypermobility, pain, neurological deficit, ankle deformity, Risser grade, and magnetic resonance imaging (MRI) findings in these patients.
Patients and methods: This cross-sectional, descriptive study included a total of 36 patients (11 males, 25 females; mean age 13.4±4.6 years; range, 6 to 24 years) with idiopathic scoliosis between January 2015 and January 2019. Data including age, sex, complaint of pain, generalized joint hypermobility (based on Beighton score), neurological deficit, ankle deformity, and definition of scoliosis were recorded. Chronological, angular, and topographic classification were carried out. The Risser grade and MRI findings were noted.
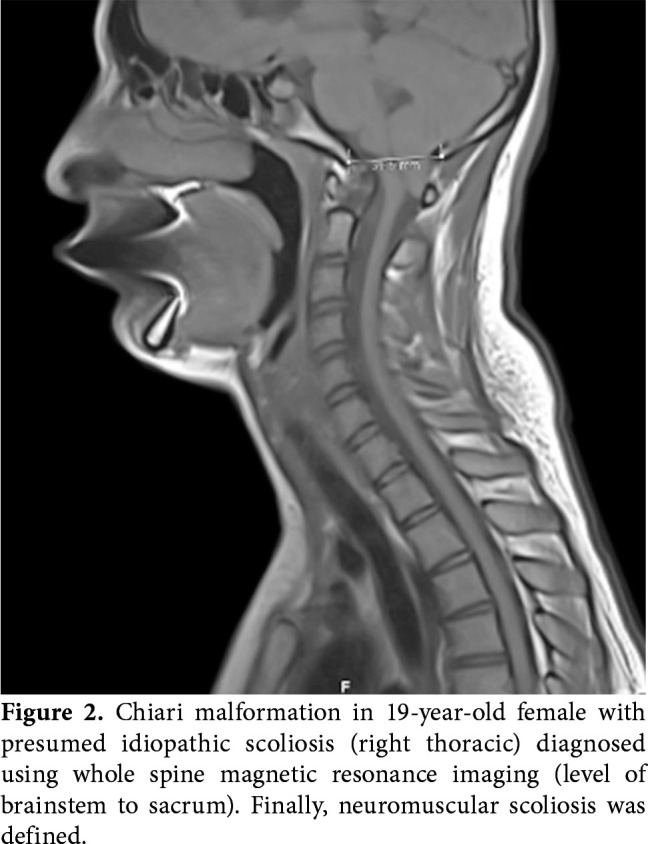
Results: Of all patients, 30 (83.3%) were idiopathic, five (13.9%) were neuromuscular, and one (2.8%) was congenital scoliosis based on MRI findings. Of 13 (36.1%) spine MRI scans, six (46.2%) were intraspinal anomalies, four were syringomyelia (30.8%), one was Chiari type 1 malformation (7.7%), and one was hemivertebrae with diastematomyelia (7.7%). The highest rates of classes according to chronological, angular, and topographical classifications of idiopathic scoliosis were adolescent (17/30, 56.7%), low angular (24/30, 80.0%), and lumbar scoliosis (15/30, 50.0%), respectively. Ten patients (33.3%) complained of pain, while 23 patients (76.7%) had no neurological deficit and seven (23.3%) had hypoesthesia. Seventeen patients (56.7%) had generalized joint hypermobility.
Conclusion: Idiopathic scoliosis with non-severe spinal deformity may present with intraspinal neural axis abnormalities, even when it is neurologically intact. Based on our study results, it seems to be useful to consider whole spine MRI for the evaluation of thoracic and lumbar scoliosis.
Keywords: Chiari; hypermobility; scoliosis; spine; syringomyelia.
Copyright © 2020, Turkish Society of Physical Medicine and Rehabilitation.
Conflict of interest statement
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Figures


Similar articles
-
The prevalence of intraspinal anomalies in infantile and juvenile patients with "presumed idiopathic" scoliosis: a MRI-based analysis of 504 patients.BMC Musculoskelet Disord. 2016 Apr 27;17:189. doi: 10.1186/s12891-016-1026-7. BMC Musculoskelet Disord. 2016. PMID: 27121616 Free PMC article.
-
Intraspinal anomalies in scoliosis: An MRI analysis of 177 consecutive scoliosis patients.Indian J Orthop. 2010 Jan;44(1):57-63. doi: 10.4103/0019-5413.58607. Indian J Orthop. 2010. PMID: 20165678 Free PMC article.
-
Intraspinal anomalies in infantile idiopathic scoliosis: prevalence and role of magnetic resonance imaging.Spine (Phila Pa 1976). 2009 May 20;34(12):E434-8. doi: 10.1097/BRS.0b013e3181a2b49f. Spine (Phila Pa 1976). 2009. PMID: 19454995
-
Intraspinal anomalies in early-onset idiopathic scoliosis.Bone Joint J. 2017 Jun;99-B(6):829-833. doi: 10.1302/0301-620X.99B6.BJJ-2016-1159.R1. Bone Joint J. 2017. PMID: 28566405 Review.
-
Prevalence and risk factors for neural axis anomalies in idiopathic scoliosis: a systematic review.Spine J. 2018 Jul;18(7):1261-1271. doi: 10.1016/j.spinee.2018.02.013. Epub 2018 Feb 14. Spine J. 2018. PMID: 29454133
Cited by
-
Preoperative Evaluation of Adolescent Idiopathic Scoliosis: The Relevance of Routine Magnetic Resonance Imaging.Cureus. 2025 Jun 14;17(6):e86003. doi: 10.7759/cureus.86003. eCollection 2025 Jun. Cureus. 2025. PMID: 40662019 Free PMC article.
-
Epidemiological and diagnostic characteristics of scoliosis in children in a single tertiary centre in Abidjan.Afr J Paediatr Surg. 2022 Jul-Sep;19(3):171-175. doi: 10.4103/ajps.AJPS_62_21. Afr J Paediatr Surg. 2022. PMID: 35775520 Free PMC article.
References
-
- Kleinberg S. The operative treatment of scoliosis. Arch Surg. 1922;5:631–645.
-
- Yılmaz H, Zateri C, Kusvuran Ozkan A, Kayalar G, Berk H. Prevalence of adolescent idiopathic scoliosis in Turkey: an epidemiological study. Spine J. 2020;20:947–955. - PubMed
-
- Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV. Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study. JAMA. 2003;289:559–567. - PubMed
LinkOut - more resources
Full Text Sources