

Understanding the impact of interruptions to HIV services during the COVID-19 pandemic: A modelling study
- PMID: 33089116
- PMCID: PMC7564522
- DOI: 10.1016/j.eclinm.2020.100483
Understanding the impact of interruptions to HIV services during the COVID-19 pandemic: A modelling study
Abstract
Background: There is concern that the COVID-19 pandemic could severely disrupt HIV services in sub-Saharan Africa. However, it is difficult to determine priorities for maintaining different elements of existing HIV services given widespread uncertainty.
Methods: We explore the impact of disruptions on HIV outcomes in South Africa, Malawi, Zimbabwe, and Uganda using a mathematical model, examine how impact is affected by model assumptions, and compare potential HIV deaths to those that may be caused by COVID-19 in the same settings.
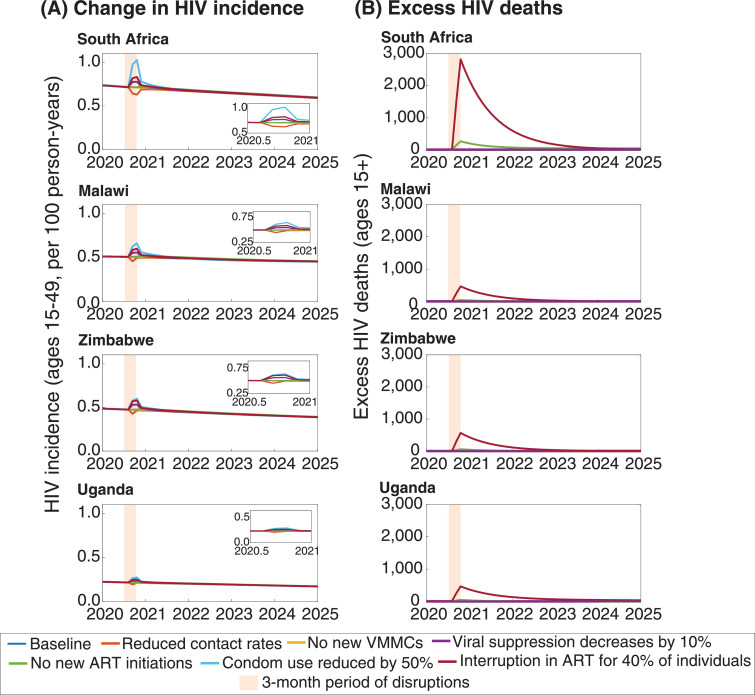
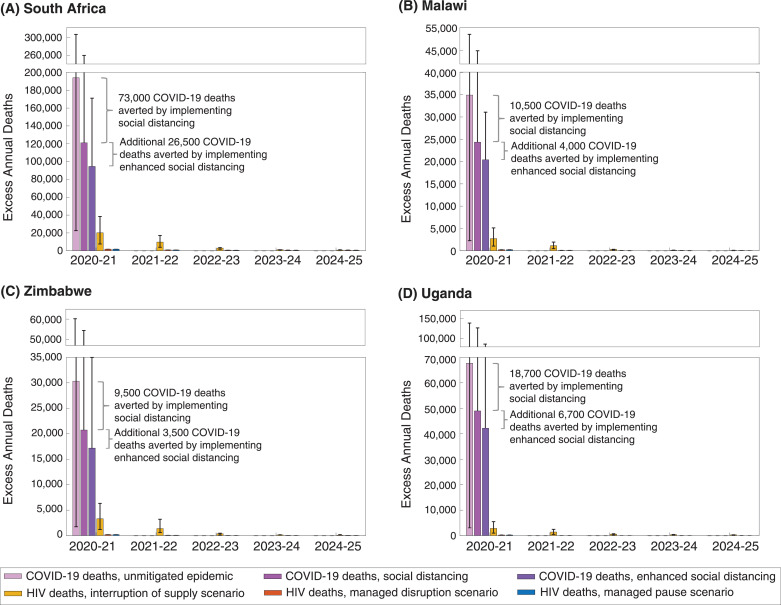
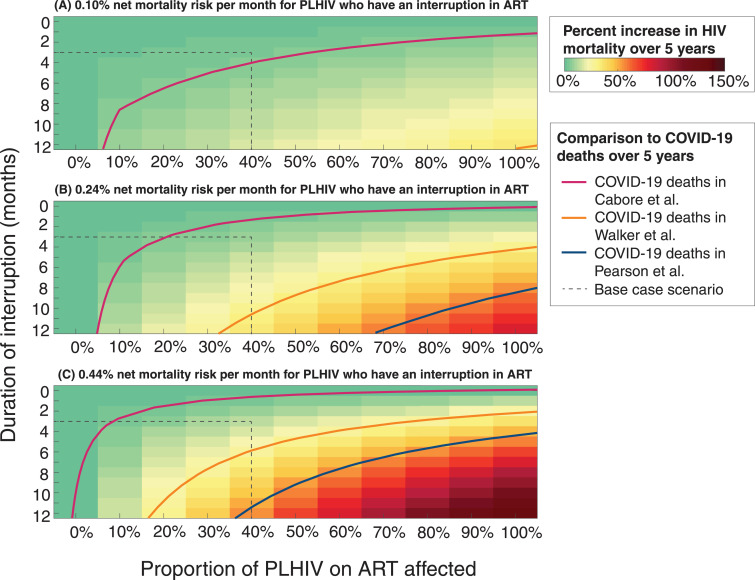
Findings: The most important determinant of HIV-related mortality is an interruption to antiretroviral treatment (ART) supply. A three-month interruption for 40% of those on ART could cause a similar number of additional deaths as those that might be saved from COVID-19 through social distancing. An interruption for more than 6-90% of individuals on ART for nine months could cause the number of HIV deaths to exceed the number of COVID-19 deaths, depending on the COVID-19 projection. However, if ART supply is maintained, but new treatment, voluntary medical male circumcision, and pre-exposure prophylaxis initiations cease for 3 months and condom use is reduced, increases in HIV deaths would be limited to <2% over five years, although this could still be accompanied by a 7% increase in new HIV infections.
Interpretation: HIV deaths could increase substantially during the COVID-19 pandemic under reasonable worst-case assumptions about interruptions to HIV services. It is a priority in high-burden countries to ensure continuity of ART during the pandemic.
Funding: Bill & Melinda Gates Foundation.
Keywords: Antiretroviral therapy; COVID-19; HIV; Mathematical modelling.
© 2020 The Authors.
Conflict of interest statement
BLJ reports personal fees from Kaiser Permanente outside the submitted work. JAS reports personal fees from the Bill and Melinda Gates Foundation and grants from USAID and the Bill and Melinda Gates Foundation outside the submitted work. TBH reports personal fees from The Global Fund, WHO and Bill & Melinda Gates Foundation outside the submitted work.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
