

Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: a matched cohort study
- PMID: 33089348
- PMCID: PMC7577365
- DOI: 10.1007/s00134-020-06281-2
Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: a matched cohort study
Abstract
Purpose: To investigate whether COVID-19-ARDS differs from all-cause ARDS.
Methods: Thirty-two consecutive, mechanically ventilated COVID-19-ARDS patients were compared to two historical ARDS sub-populations 1:1 matched for PaO2/FiO2 or for compliance of the respiratory system. Gas exchange, hemodynamics and respiratory mechanics were recorded at 5 and 15 cmH2O PEEP. CT scan variables were measured at 5 cmH2O PEEP.
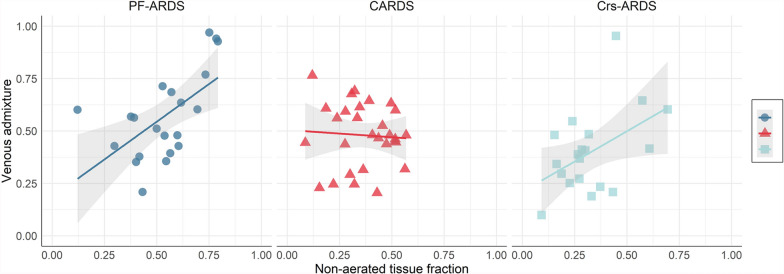
Results: Anthropometric characteristics were similar in COVID-19-ARDS, PaO2/FiO2-matched-ARDS and Compliance-matched-ARDS. The PaO2/FiO2-matched-ARDS and COVID-19-ARDS populations (both with PaO2/FiO2 106 ± 59 mmHg) had different respiratory system compliances (Crs) (39 ± 11 vs 49.9 ± 15.4 ml/cmH2O, p = 0.03). The Compliance-matched-ARDS and COVID-19-ARDS had similar Crs (50.1 ± 15.7 and 49.9 ± 15.4 ml/cmH2O, respectively) but significantly lower PaO2/FiO2 for the same Crs (160 ± 62 vs 106.5 ± 59.6 mmHg, p < 0.001). The three populations had similar lung weights but COVID-19-ARDS had significantly higher lung gas volume (PaO2/FiO2-matched-ARDS 930 ± 644 ml, COVID-19-ARDS 1670 ± 791 ml and Compliance-matched-ARDS 1301 ± 627 ml, p < 0.05). The venous admixture was significantly related to the non-aerated tissue in PaO2/FiO2-matched-ARDS and Compliance-matched-ARDS (p < 0.001) but unrelated in COVID-19-ARDS (p = 0.75), suggesting that hypoxemia was not only due to the extent of non-aerated tissue. Increasing PEEP from 5 to 15 cmH2O improved oxygenation in all groups. However, while lung mechanics and dead space improved in PaO2/FiO2-matched-ARDS, suggesting recruitment as primary mechanism, they remained unmodified or worsened in COVID-19-ARDS and Compliance-matched-ARDS, suggesting lower recruitment potential and/or blood flow redistribution.
Conclusions: COVID-19-ARDS is a subset of ARDS characterized overall by higher compliance and lung gas volume for a given PaO2/FiO2, at least when considered within the timeframe of our study.
Keywords: ARDS; COVID-19; CT scan; Mechanical ventilation; Respiratory system mechanics.
Conflict of interest statement
The authors have no interests to disclose.
Figures


Comment in
-
Is severe COVID-19 pneumonia a typical or atypical form of ARDS? And does it matter?Intensive Care Med. 2021 Jan;47(1):83-85. doi: 10.1007/s00134-020-06320-y. Epub 2020 Nov 25. Intensive Care Med. 2021. PMID: 33237346 Free PMC article. No abstract available.
-
Anatomical, physiological and clinical similarities and differences in ARDS physiological subtypes.Intensive Care Med. 2021 Apr;47(4):493-494. doi: 10.1007/s00134-021-06348-8. Epub 2021 Feb 2. Intensive Care Med. 2021. PMID: 33527154 Free PMC article. No abstract available.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
