

The role of damage control surgery in the treatment of perforated colonic diverticulitis: a systematic review and meta-analysis
- PMID: 33089382
- PMCID: PMC8026449
- DOI: 10.1007/s00384-020-03784-8
The role of damage control surgery in the treatment of perforated colonic diverticulitis: a systematic review and meta-analysis
Abstract
Introduction: Damage control surgery (DCS) is the classic approach to manage severe trauma and has recently also been considered an appropriate approach to the treatment of critically ill patients with severe intra-abdominal sepsis. The purpose of the present review is to evaluate the outcomes following DCS for Hinchey II-IV complicated acute diverticulitis (CAD).
Methods: A comprehensive systematic search was undertaken to identify all randomized clinical trials (RCTs) and observational studies, irrespectively of their size, publication status, and language. Adults who have undergone DCS for CAD Hinchey II, III, or IV were included in this review. DCS is compared with the immediate and definitive surgical treatment in the form of HP, colonic resection, and primary anastomosis (RPA) with or without covering stoma or laparoscopic lavage. We searched the following electronic databases: PubMed MEDLINE, Scopus, and ISI Web of Knowledge. The protocol of this systematic review and meta-analysis was published on Prospero (CRD42020144953).
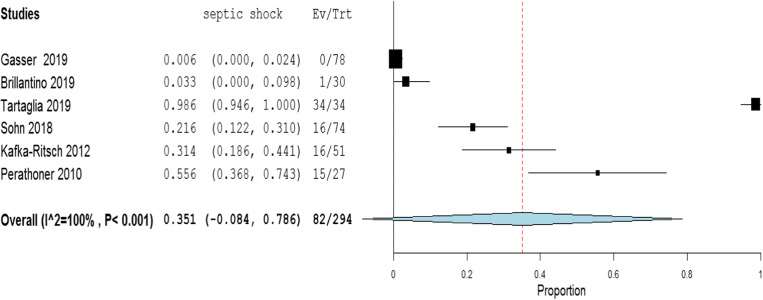
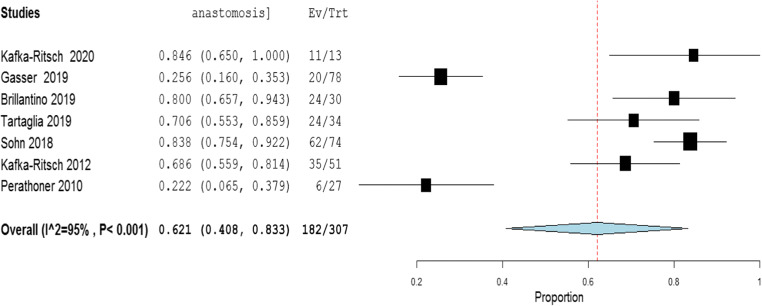
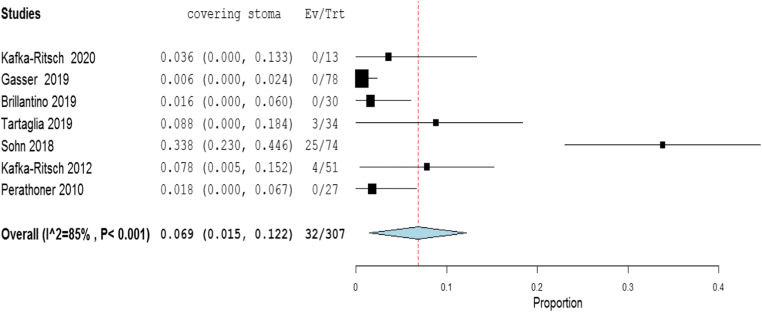
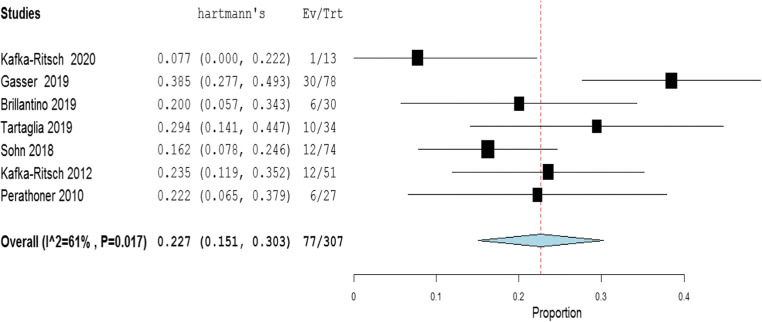
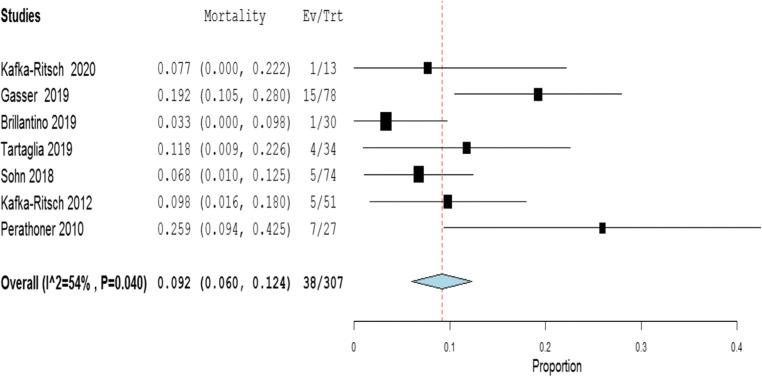
Results: Nine studies with 318 patients, undergoing DCS, were included. The presence of septic shock at the presentation in the emergency department was heterogeneous, and the weighted mean rate of septic shock across the studies was shown to be 35.1% [95% CI 8.4 to 78.6%]. The majority of the patients had Hinchey III (68.3%) disease. The remainder had either Hinchey IV (28.9%) or Hinchey II (2.8%). Phase I is similarly described in most of the studies as lavage, limited resection with closed blind colonic ends. In a few studies, resection and anastomosis (9.1%) or suture of the perforation site (0.9%) were performed in phase I of DCS. In those patients who underwent DCS, the most common method of temporary abdominal closure (TAC) was the negative pressure wound therapy (NPWT) (97.8%). The RPA was performed in 62.1% [95% CI 40.8 to 83.3%] and the 22.7% [95% CI 15.1 to 30.3%]: 12.8% during phase I and 87.2% during phase III. A covering ileostomy was performed in 6.9% [95% CI 1.5 to 12.2%]. In patients with RPA, the overall leak was 7.3% [95% CI 4.3 to 10.4%] and the major anastomotic leaks were 4.7% [95% CI 2.0 to 7.4%]; the rate of postoperative mortality was estimated to be 9.2% [95% CI 6.0 to 12.4%].
Conclusions: The present meta-analysis revealed an approximately 62.1% weighted rate of achieving GI continuity with the DCS approach to generalized peritonitis in Hinchey III and IV with major leaks of 4.7% and overall mortality of 9.2%. Despite the promising results, we are aware of the limitations related to the significant heterogeneity of inclusion criteria. Importantly, the low rate of reported septic shock may point toward selection bias. Further studies are needed to evaluate the clinical advantages and cost-effectiveness of the DCS approach.
Keywords: Damage control surgery; Diverticular perforation; Diverticular peritonitis.
Figures



References
-
- Mikulicz J. Weitere Erfahrungen über die operative Behandlung der Perforationsperitonitis. Langenbecks Arch Chir. 1889;39:75.
-
- Kirschner М. Die Behandlung der akuten eitrigen freien Bauchfellentzündung. Langebeck Arch Chir. 1926;142:53–67.
-
- Gloor B, Worni M, Büchler MW. Diffuse Peritonitis. In: Schein M, Marshall JC, editors. Source Control: A Guide to the Management of Surgical Infections. Berlin Heidelberg: Springer-Verlag; 2003. pp. 87–91.
-
- Sartelli M, Catena F, Abu-Zidan FM, Ansaloni L, Biffl WL, Boermeester MA, Ceresoli M, Chiara O, Coccolini F, de Waele JJ, di Saverio S, Eckmann C, Fraga GP, Giannella M, Girardis M, Griffiths EA, Kashuk J, Kirkpatrick AW, Khokha V, Kluger Y, Labricciosa FM, Leppaniemi A, Maier RV, May AK, Malangoni M, Martin-Loeches I, Mazuski J, Montravers P, Peitzman A, Pereira BM, Reis T, Sakakushev B, Sganga G, Soreide K, Sugrue M, Ulrych J, Vincent JL, Viale P, Moore EE. Management of intra-abdominal infections: recommendations by the WSES 2016 consensus conference. World J Emerg Surg. 2017;12:22. - PMC - PubMed
-
- Hecker A, Uhle F, Schwandner T, Padberg W, Weigand MA. Diagnostics, therapy and outcome prediction in abdominal sepsis: current standarts and future perspectives. Langenbecks Arch Surg. 2014;399:11–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
