

The beneficial impact of cardiac rehabilitation on obstructive sleep apnea in patients with coronary artery disease
- PMID: 33089775
- PMCID: PMC7927323
- DOI: 10.5664/jcsm.8900
The beneficial impact of cardiac rehabilitation on obstructive sleep apnea in patients with coronary artery disease
Abstract
Study objectives: To assess the impact of cardiac rehabilitation for decreasing sleep-disordered breathing in patients with coronary artery disease.
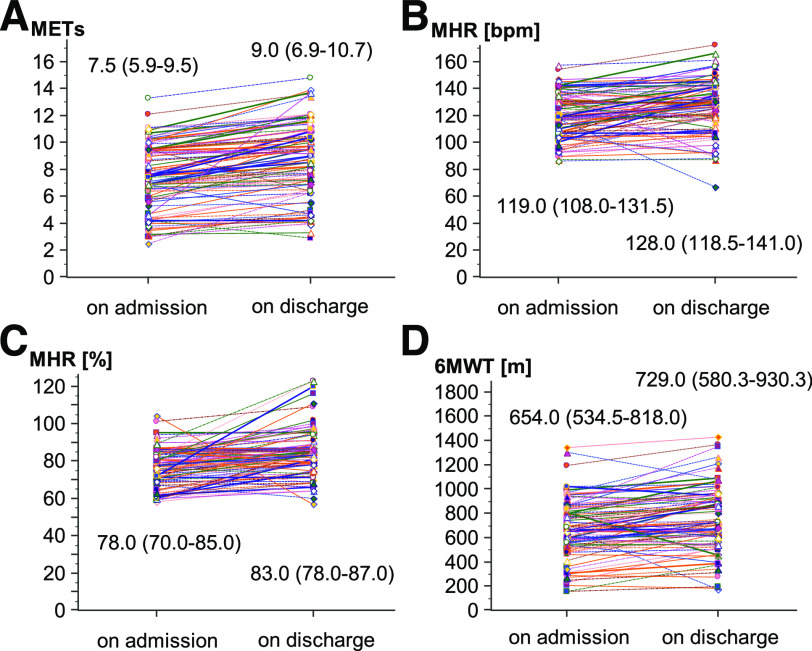
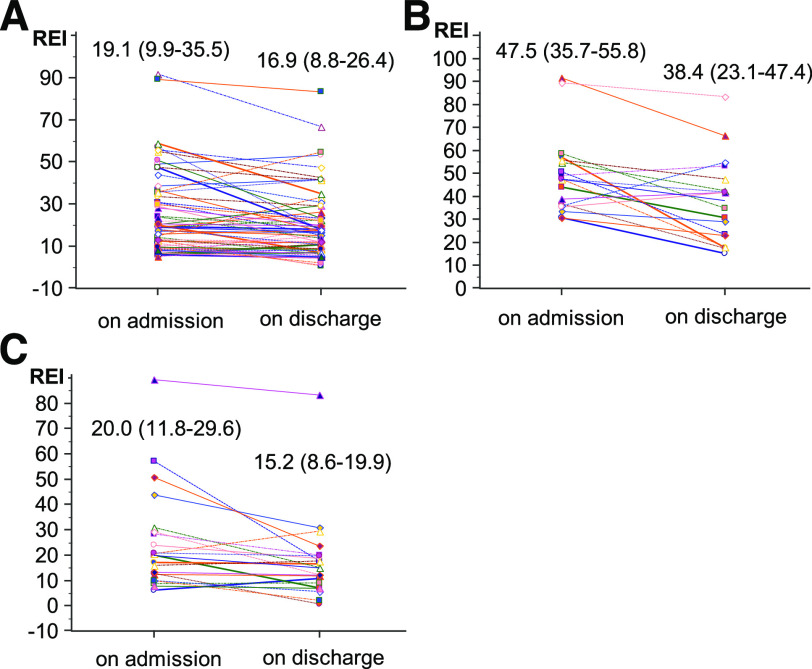
Methods: The study included 121 patients aged 60.01 ± 10.08 years, 101 of whom were men, with an increased pretest probability of OSA. The cardiac rehabilitation program lasted 21-25 days. The improvement in cardiorespiratory fitness was assessed using the changes in peak metabolic equivalents, the maximal heart rate achieved, the proportion of the age- and sex-predicted maximal heart rate, and the Six-Minute Walk Test distance. Level 3 portable sleep tests with respiratory event index assessments were performed in 113 patients on admission and discharge.
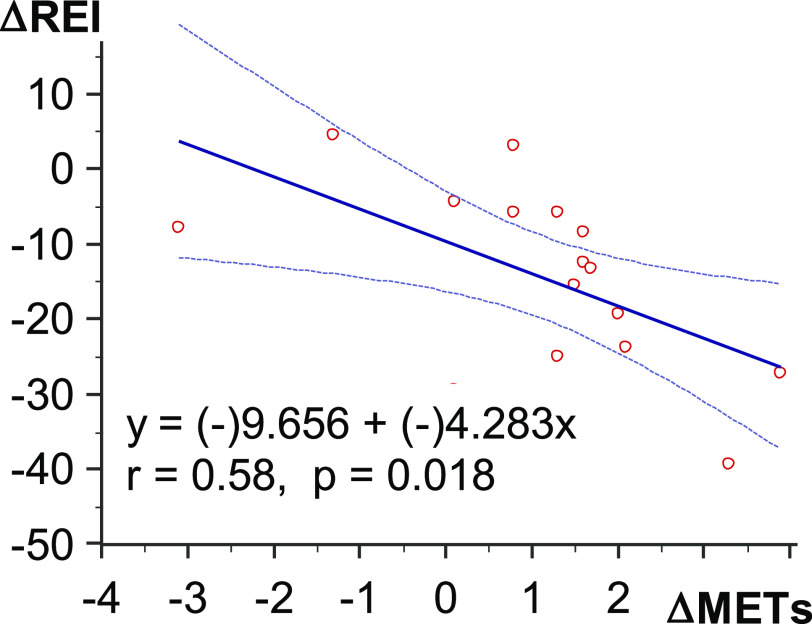
Results: Increases were achieved in metabolic equivalents (Δ1.20; 95% confidence interval [CI], 0.95-1.40; P < .0001), maximal heart rate (-Δ7.5 beats per minute; 95% CI, 5.00-10.50; P < .0001), proportion of age- and sex-predicted maximal heart rate (Δ5.50%; 95% CI, 4.00-7.50; P < .0001), and the Six-Minute Walk Test distance (Δ91.00 m; 95% CI, 62.50-120.00; P < .0001). Sleep-disordered breathing was diagnosed in 94 (83.19%) patients: moderate in 28 (24.8%) patients and severe in 27 (23.9%) patients, with a respiratory event index of 19.75 (interquartile range, 17.20-24.00) and 47.50 (interquartile range, 35.96-56.78), respectively. OSA was dominant in 90.40% of patients. The respiratory event index reduction achieved in the sleep-disordered breathing group was -Δ3.65 (95% CI, -6.30 to -1.25; P = .003) and was in parallel to the improvement in cardiorespiratory fitness in the subgroups with the highest effort load and with severe sleep-disordered breathing: -Δ6.40 (95% CI, -11.40 to -1.90; P = .03) and -Δ11.00 (95% CI, -18.65 to -4.40; P = .003), respectively.
Conclusions: High-intensity exercise training during cardiac rehabilitation resulted in a significant decrease in OSA, when severe, in parallel with an improvement in cardiorespiratory fitness in patients with coronary artery disease.
Keywords: OSA; cardiac rehabilitation; cardiorespiratory fitness; coronary artery disease.
© 2021 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. Work for this study was performed at the Department of Electrocardiology and Heart Failure, Medical University of Silesia, Katowice, Poland. The authors report no conflicts of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
