

Echocardiographic abnormalities and predictors of mortality in hospitalized COVID-19 patients: the ECHOVID-19 study
- PMID: 33089972
- PMCID: PMC7755011
- DOI: 10.1002/ehf2.13044
Echocardiographic abnormalities and predictors of mortality in hospitalized COVID-19 patients: the ECHOVID-19 study
Abstract
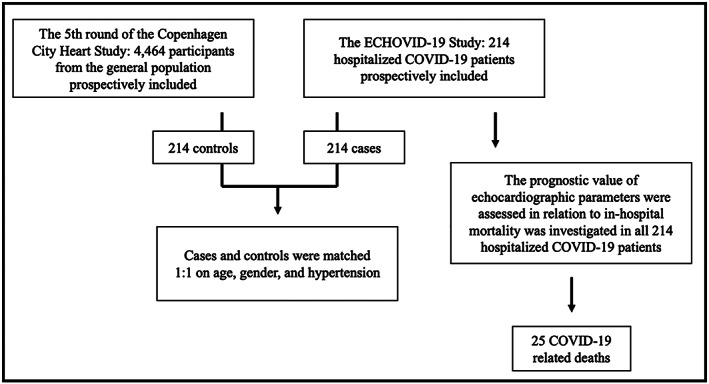
Aims: The present study had two aims: (i) compare echocardiographic parameters in COVID-19 patients with matched controls and (2) assess the prognostic value of measures of left (LV) and right ventricular (RV) function in relation to COVID-19 related death.
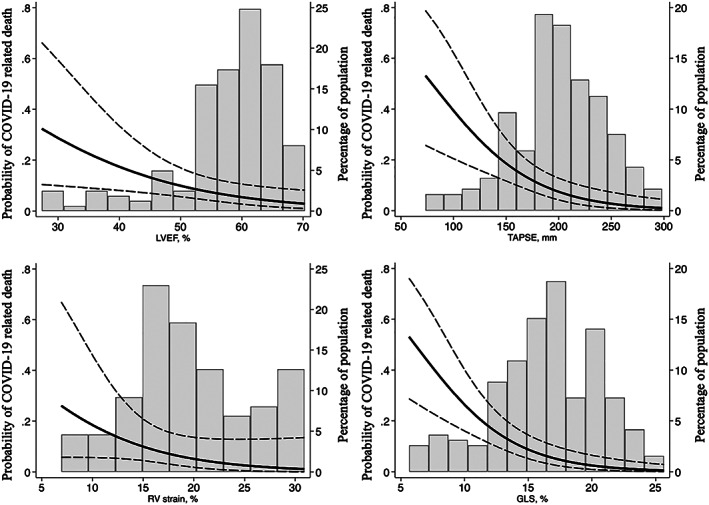
Methods and results: In this prospective multicentre cohort study, 214 consecutive hospitalized COVID-19 patients underwent an echocardiographic examination (by pre-determined research protocol). All participants were successfully matched 1:1 with controls from the general population on age, sex, and hypertension. Mean age of the study sample was 69 years, and 55% were male participants. LV and RV systolic function was significantly reduced in COVID-19 cases as assessed by global longitudinal strain (GLS) (16.4% ± 4.3 vs. 18.5% ± 3.0, P < 0.001), tricuspid annular plane systolic excursion (TAPSE) (2.0 ± 0.4 vs. 2.6 ± 0.5, P < 0.001), and RV strain (19.8 ± 5.9 vs. 24.2 ± 6.5, P = 0.004). All parameters remained significantly reduced after adjusting for important cardiac risk factors. During follow-up (median: 40 days), 25 COVID-19 cases died. In multivariable Cox regression reduced TAPSE [hazard ratio (HR) = 1.18, 95% confidence interval (CI) [1.07-1.31], P = 0.002, per 1 mm decrease], RV strain (HR = 1.64, 95%CI[1.02;2.66], P = 0.043, per 1% decrease) and GLS (HR = 1.20, 95%CI[1.07-1.35], P = 0.002, per 1% decrease) were significantly associated with COVID-19-related death. TAPSE and GLS remained significantly associated with the outcome after restricting the analysis to patients without prevalent heart disease.
Conclusions: RV and LV function are significantly impaired in hospitalized COVID-19 patients compared with matched controls. Furthermore, reduced TAPSE and GLS are independently associated with COVID-19-related death.
Keywords: COVID-19; Echocardiography; Global longitudinal strain; Right ventricular strain; SARS-CoV-2.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
T.B.S. reports receiving research grants from Sanofi Pasteur, and GE Healthcare, is a Steering Committee member of the Amgen financed GALACTIC‐HF trial, on advisory boards for Sanofi Pasteur and Amgen, and speaker honorariums from Novartis and Sanofi Pasteur. The remaining authors have nothing to disclose.
Figures
References
-
- Mahase E. Coronavirus covid‐19 has killed more people than SARS and MERS combined, despite lower case fatality rate. BMJ 2020; 368: m641. - PubMed
-
- Guan W‐J, Ni Z‐Y, Hu Y, Liang W‐H, Ou C‐Q, He J‐X, Liu L, Shan H, Lei C‐L, Hui DSC, Du B, Li L‐J, Zeng G, Yuen K‐Y, Chen R‐C, Tang C‐L, Wang T, Chen P‐Y, Xiang J, Li S‐Y, Wang J‐L, Liang Z‐J, Peng Y‐X, Wei L, Liu Y, Hu Y‐H, Peng P, Wang J‐M, Liu J‐Y, Chen Z. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020; 382: 1708–1720. - PMC - PubMed
-
- Chapman AR, Bularga A, Mills NL. High‐sensitivity cardiac troponin can be An ally in the fight against COVID‐19. Circulation 2020; 141: 1733–1735. - PubMed
-
- Alpert JS. The effect of right ventricular dysfunction on left ventricular form and function. Chest 2001; 119: 1632–1633. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
