

The effect of blood transfusion on outcomes among African children admitted to hospital with Plasmodium falciparum malaria: a prospective, multicentre observational study
- PMID: 33091354
- PMCID: PMC7611367
- DOI: 10.1016/S2352-3026(20)30288-X
The effect of blood transfusion on outcomes among African children admitted to hospital with Plasmodium falciparum malaria: a prospective, multicentre observational study
Abstract
Background: Infection with Plasmodium falciparum leads to severe malaria and death in approximately 400 000 children each year in sub-Saharan Africa. Blood transfusion might benefit some patients with malaria but could potentially harm others. The aim of this study was to estimate the association between transfusion and death among children admitted to hospital with P falciparum malaria.
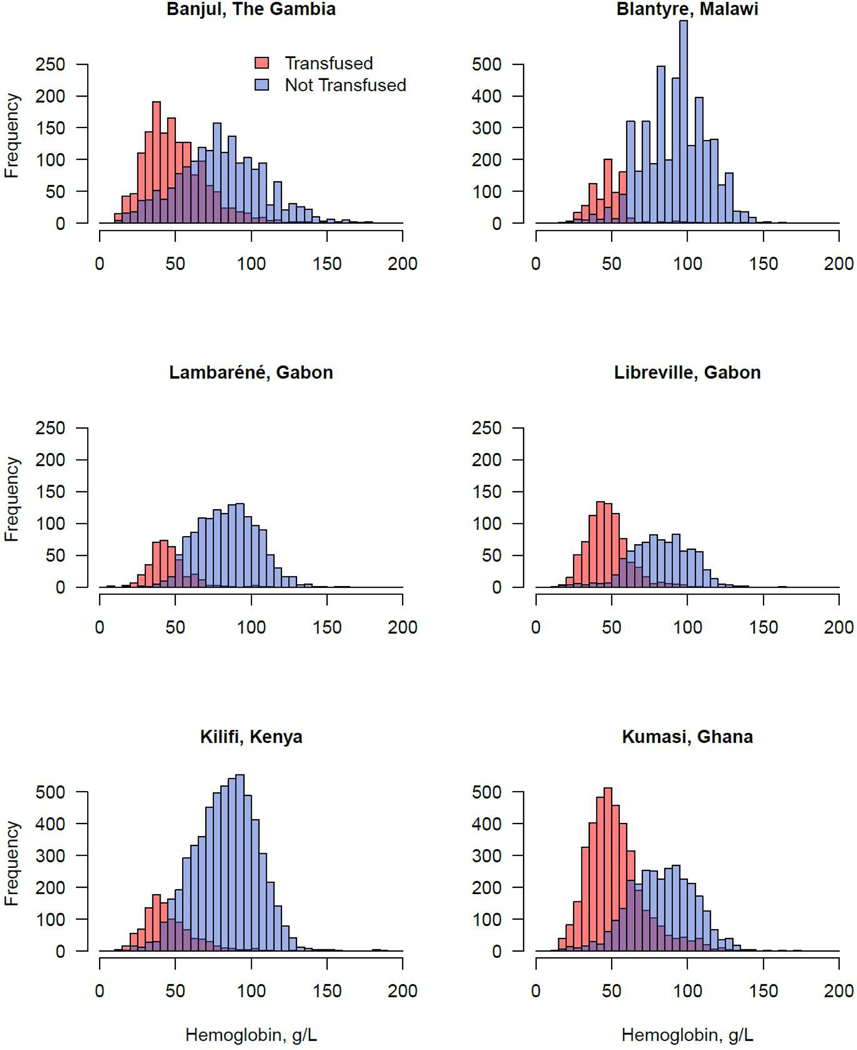
Methods: In this prospective, multicentre observational study, we analysed admissions to six tertiary care hospitals in The Gambia, Malawi, Gabon, Kenya, and Ghana that participated in the Severe Malaria in African Children network. Patients were enrolled if they were younger than 180 months and had a Giemsa-stained thick blood smear that was positive for P falciparum. Blood transfusion (whole blood at a target volume of 20 mL per kg) was administered at the discretion of the responsible physicians who were aware of local and international transfusion guidelines. The primary endpoint was death associated with transfusion, which was estimated using models adjusted for site and disease severity. We also aimed to identify factors associated with the decision to transfuse. The exploratory objective was to estimate optimal haemoglobin transfusion thresholds using generalised additive models.
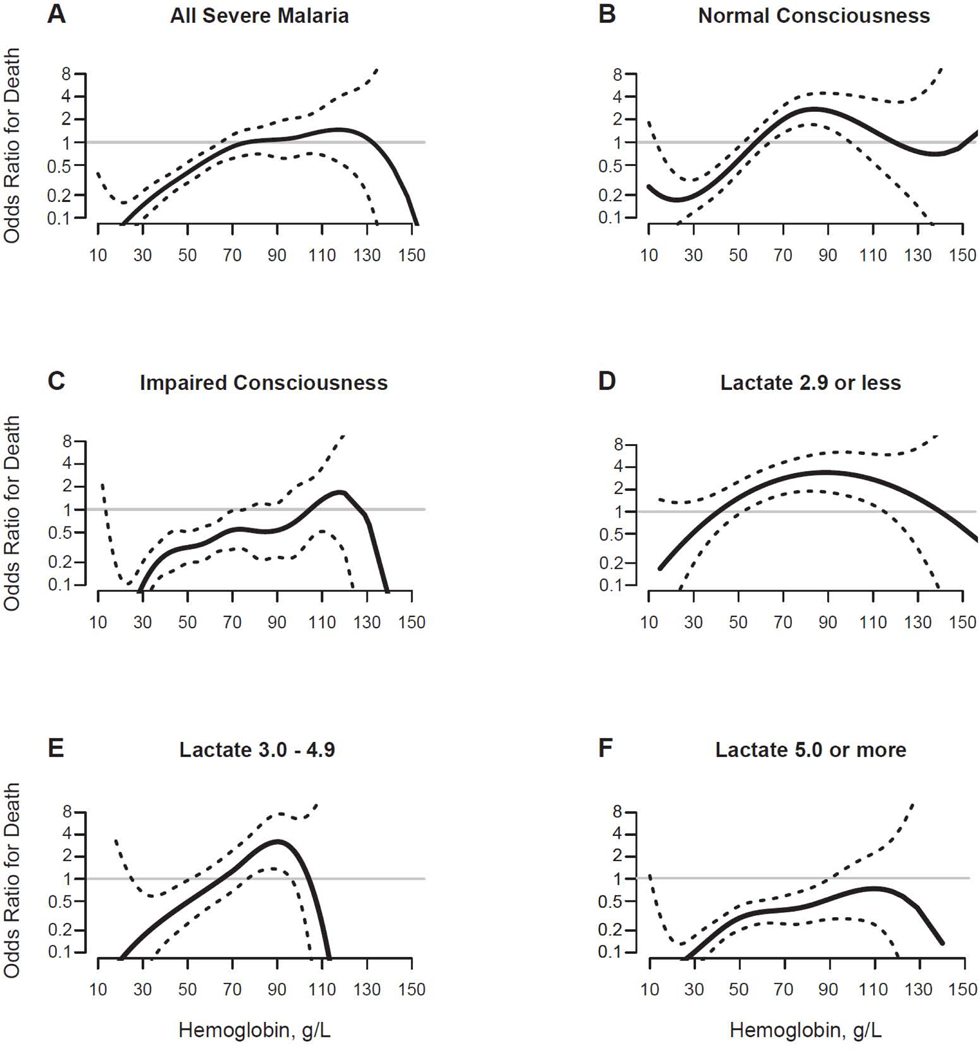
Findings: Between Dec 19, 2000, and March 8, 2005, 26 106 patients were enrolled in the study, 25 893 of whom had their transfusion status recorded and were included in the primary analysis. 8513 (32·8%) patients received a blood transfusion. Patients were followed-up until discharge from hospital for a median of 2 days (IQR 1-4). 405 (4·8%) of 8513 patients who received a transfusion died compared with 689 (4·0%) of 17 380 patients who did not receive a transfusion. Transfusion was associated with decreased odds of death in site-adjusted analysis (odds ratio [OR] 0·82 [95% CI 0·71-0·94]) and after adjusting for the increased disease severity of patients who received a transfusion (0·50 [0·42-0·60]). Severe anaemia, elevated lactate concentration, respiratory distress, and parasite density were associated with greater odds of receiving a transfusion. Among all study participants, transfusion was associated with improved survival when the admission haemoglobin concentration was up to 77 g/L (95% CI 65-110). Among those with impaired consciousness (Blantyre Coma Score ≤4), transfusion was associated with improved survival at haemoglobin concentrations up to 105 g/L (95% CI 71-115). Among those with hyperlactataemia (blood lactate ≥5·0 mmol/L), transfusion was not significantly associated with harm at any haemoglobin concentration-ie, the OR of death comparing transfused versus not transfused was less than 1 at all haemoglobin concentrations (lower bound of the 95% CI for the haemoglobin concentration at which the OR of death equals 1: 90 g/L; no upper bound).
Interpretation: Our findings suggest that whole blood transfusion was associated with improved survival among children hospitalised with P falciparum malaria. Among those with impaired consciousness or hyperlactataemia, transfusion was associated with improved survival at haemoglobin concentrations above the currently recommended transfusion threshold. These findings highlight the need to do randomised controlled trials to test higher transfusion thresholds among African children with severe malaria complicated by these factors.
Funding: US National Institute of Allergy and Infectious Diseases.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Time-to-death is a potential confounder in observational studies of blood transfusion in severe malaria - Authors' reply.Lancet Haematol. 2021 Jan;8(1):e12-e13. doi: 10.1016/S2352-3026(20)30412-9. Epub 2020 Dec 22. Lancet Haematol. 2021. PMID: 33357473 Free PMC article. No abstract available.
-
Time-to-death is a potential confounder in observational studies of blood transfusion in severe malaria.Lancet Haematol. 2021 Jan;8(1):e12. doi: 10.1016/S2352-3026(20)30395-1. Epub 2020 Dec 22. Lancet Haematol. 2021. PMID: 33357474 No abstract available.
References
-
- World malaria report 2019. https://www.who.int/publications-detail/world-malaria-report-2019 (accessed Feb 11, 2020).
-
- Molyneux ME, Taylor TE, Wirima JJ, Borgstein A. Clinical features and prognostic indicators in paediatric cerebral malaria: a study of 131 comatose Malawian children. Q J Med 1989; 71: 441–59. - PubMed
-
- Marsh K, Forster D, Waruiru C, et al. Indicators of life-threatening malaria in African children. N Engl J Med 1995; 332: 1399–404. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
